
Sauna For Prevention of Cardiovascular & Alzheimer’s Disease & For Detoxification
Dr. Jari Laukkanen on Sauna Use For the Prevention of Cardiovascular & Alzheimer’s Disease
This podcast features Jari Laukkanen, M.D., Ph.D., a cardiologist and scientist at the Institute of Public Health and Clinical Nutrition, University of Eastern Finland, Kuopio. Dr. Laukkanen has been conducting long-term trials looking at the health effects of sauna use in a population of over 2,000 middle-aged men in Finland. The results? Massive reductions in mortality and memory disease in a dose-response fashion at 20-year follow-up. In this almost 25-minute episode, we talk about…
- 00:00:37 – The association between sauna use and fatal cardiovascular outcomes
- 00:00:37 – The inverse association between cardiovascular-related deaths and all-cause deaths.
- 00:02:00 – How men that used the sauna 2-3 times per week had a 27% lower cardiovascular-related mortality than men that used the sauna 1 time per week
- 00:02:15 – How men that used the sauna 4-7 times per week had a 50% lower cardiovascular-related mortality than men that used the sauna one time per week.
- 00:02:50 – The confounding factors Dr. Laukkanen and his colleagues had to adjust for, such as physical exercise, cholesterol, obesity, smoking, alcohol consumption, socioeconomic status.
- 00:03:26 – The various types of cardiac-related deaths their reductions were shown in, including coronary artery disease, sudden cardiac death and more.
- 00:05:00 – How one of the major mechanisms by which sauna use improves heart health is by reducing blood pressure and incident hypertension.
- 00:05:40 – The mechanisms by which the sauna lowers blood pressure, which can occur via balancing of the autonomic nervous system, improvements in blood vessel function, decreases in arterial stiffness and compliance of arteries.
- 00:06:17 – The increases in heart rate seen with sauna use that make it similar to moderate aerobic exercise in some ways (up to 150 beats/min!).
- 00:06:56 – How time spent in the sauna was one of the more important factors for risk reduction with at least 20 minutes per session in a 174 F (79C) 4-7 times per week being a “sweet spot.”
- 00:09:29 – The inverse, dose-response relationship between sauna use and all-cause mortality: 24% for 2-3 times per week, 40% for 4-7 times.
- 00:10:00 – His newest study that now shows a reduction in risk in a similar dose-response fashion for dementia and Alzheimer’s disease by around 65% for the most frequent sauna users.
- 00:10:18 – The way sauna use increases heat shock proteins which repair damaged proteins and prevent protein aggregates and how this could end up being at least one potential molecular mechanism at play.
- 00:13:03 – How sauna use increases growth hormone by 200-330%.
- 00:14:10 – The patterns of sauna use and especially whether to sauna before or after you weight train.
- 00:15:55 – The effect of sauna on mood which may be from improvements in cardiorespiratory fitness and possibly endorphins as well.
- 00:18:39 – How sauna improves heart rate variability.
- 00:20:04 – Cold-water immersion after sauna and a few cautionary words for extreme contrast therapy in people with a pre-existing heart condition that is currently unstable.
Further, Dr. Mary Shackelton, MPH, ND talks about skin as a pathway for detoxification and how important it is to sweat on a weekly basis. Infrared saunas are one of the most effective ways of releasing toxins from deep within one’s tissues.
__________________
For more: https://madisonarealymesupportgroup.com/2019/03/31/how-to-detox-naturally-for-healthy-aging/
https://madisonarealymesupportgroup.com/2015/12/06/tips-for-newbies/
https://madisonarealymesupportgroup.com/2019/01/26/lyme-herxheimer-reactions-dr-rawls/
https://madisonarealymesupportgroup.com/2018/02/24/top-3-lyme-detox-myths-busted-dr-rawls/
https://madisonarealymesupportgroup.com/2018/03/02/dmso-msm-for-lyme-msids/
https://madisonarealymesupportgroup.com/2018/01/03/the-invisible-universe-of-the-human-microbiome-msm/ Briefly, MSM stands for Methylsulfonylmethane and is 34% sulfur by weight. Sulfur plays a crucial role in detoxification and is an important antioxidant for producing glutathione. If you aren’t getting enough sulfur, glutathione can not work. Even if you have a diet rich in sulfur (think cabbage, onions, garlic, broccoli, etc – essentially the stinky veggies – and many other food items as well) your body still could use supplementation.
https://madisonarealymesupportgroup.com/2019/03/14/melatonin-benefits-uses/ Besides helping sleep, melatonin is known for protecting the brain. Research has shown starting to supplement in middle age protects against Alzheimer’s, reduces the risk of Parkinson’s, shrinks the size of the infarct area in a stroke, minimizes brain swelling & dysfunction after head injury, and increases the “longevity protein” SIRT1.









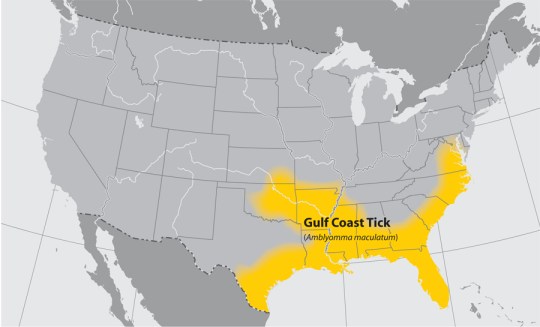
 Tick distribution maps found:
Tick distribution maps found: 