
There’s a New Type of Lyme Disease in NY. OY.
https://medicaldetective.substack.com/p/theres-a-new-type-of-lyme-disease-in-new-york-state-oy
There’s A New Type of Lyme disease in New York State. Oy.
Jun 10, 2026

There are very few headlines that catch my eye. This one was surprising but not unexpected, since ticks are known to spread via travel on birds (and air travel has become more expensive these days, as I just found out after booking several flights). Here is the news release that made me pay more attention:
So what exactly is the ‘new type of Lyme disease (LD)’? It’s a strain of LD that is not normally found in NY State. Its Borrelia mayonii. The CDC just reported on it in their MMWR report. Here is a brief summary:
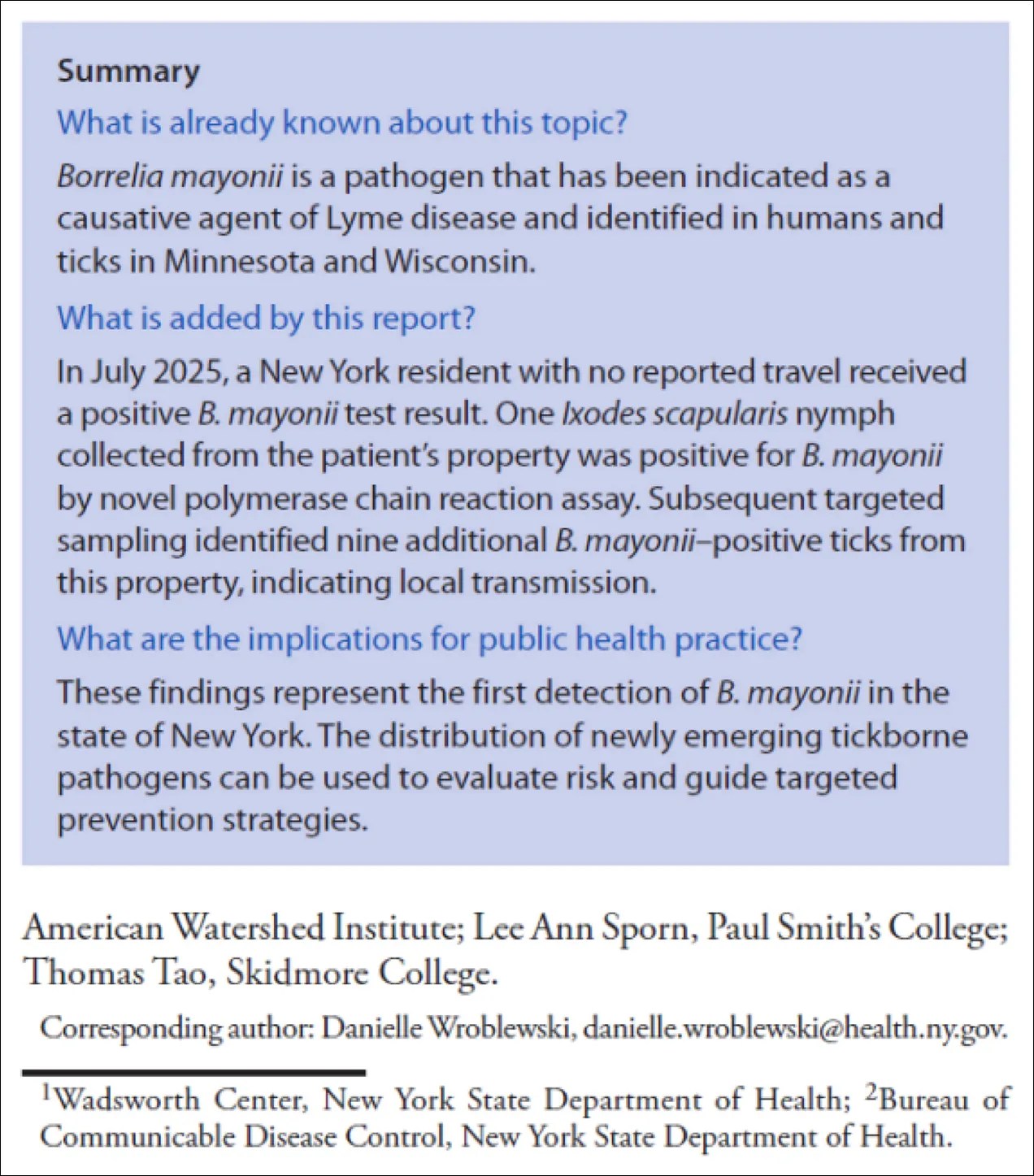
[From: Nafiz TN, Prusinski MA, Gubbala S, et al. Notes from the Field: Borrelia mayonii Lyme Disease — New York, 2025. MMWR Morb Mortal Wkly Rep 2026;75:271–272. DOI: http://dx.doi.org/10.15585/mmwr.mm7521a2]
This is an important case study, because B. mayonii clinically presents differently than an infection with Borrelia burgdorferi (Bb), so we need to understand how to properly diagnose and treat it if it is being found in new areas. (See link for article)
________________
**Comment**
Dr. Horowitz points out that the rash with B. mayonii is not the ‘classic’ rash seen with Bb, which isn’t so classic either, and highly variable – although it’s completely diagnostic, proving infection – no testing even required. If you have the rash, you are infected, period.
But there is concern for more severe systemic illness with B. mayonii due to a high level of spirochetes in the blood.
For more:
- https://madisonarealymesupportgroup.com/2017/07/18/transmission-time-for-borrelia-mayonii-by-nymphal-ticks-mouse-model/
- https://madisonarealymesupportgroup.com/2024/12/31/medical-detective-4-how-to-survive-in-a-tick-filled-world/
- https://www.cdc.gov/mmwr/volumes/75/wr/mm7521a2.htm Identified in humans and ticks in Minnesota and Wisconsin
