
https://flccc.substack.com/p/the-together-trial-was-designed-to
The TOGETHER Trial Was Designed to Fail
Big Pharma has been sponsoring trials to discredit cheap generic treatments for COVID since the earliest days of the pandemic.
 |

If you read anything about the TOGETHER trial in the past few weeks (and you didn’t read it here) chances are you heard the tired trope that ivermectin doesn’t work.
When the study was published, the media urgently blasted out clickbait headlines to this effect, uncritically rehashing Big Pharma propaganda. The Wall Street Journal blared “Ivermectin Didn’t Reduce Covid-19 Hospitalizations in Largest Trial to Date” and The New York Times trumpeted, “Ivermectin Does Not Reduce Risk of Covid Hospitalization, Large Study Finds.”
The problem, as ever, is that the study was designed to fail. In a piece published by The Brownstone Institute, Dr. Pierre Kory highlights the study’s flaws:
There were no explicit exclusion criteria for trial participants on ivermectin, meaning both trial groups had access to the same drug. This is an indefensible omission given that in Brazil, where the trial was conducted, ivermectin is available over-the-counter and widely used.
The treatment window was set for only three days, an obvious “tell” of underdosing given, for example, that both Merck’s molnupiravir and Pfizer’ Paxlovid require five days. The trial actually started out testing only a single dose, presumably until the investigators realized they could never disprove anything with that regimen.
And the trial was conducted during the throes of the massive gamma variant surge, one of the most virulent and deadly COVID variants. The dosage of the trial was far lower than everyday Brazilian clinicians were prescribing patients at the time to match the strength of the strain.
It’s amazing to see so many powerful headlines for such a half-baked study, when a similar, far larger study published in January showing ivermectin led to massive reductions in COVID infection, hospitalization and mortality received virtually no media coverage.
But this is nothing new. Big Pharma has been sponsoring trials to discredit cheap generic treatments for COVID since the earliest days of the pandemic. It has addicted media companies to its bottom-line well of advertising cash, ensuring the study results are blindly parroted all over the Internet to reinforce the company line: more expensive treatments and vaccines work, cheap generic alternatives don’t. Social media companies, just as drunk on power and pharma cash, censor and shut down all dissent.
Pierre highlights a particularly aggravating example:
Clicking on a Reddit thread featuring MDs, PhDs and public health professionals discussing the randomization of the TOGETHER trial first brings users to an ominous page with a “quarantine” caveat, urging readers to “please consult your physician.”
The most grotesque perversions imaginable are readily available to any child on the Internet, but informed medical conversations come with a warning label.
Using fear to force doctors to toe the line
The TOGETHER trial is just another step on the way to destroying doctors who don’t toe the company line. California Democrats are pushing legislation (Assembly Bill 2098) that would grant the state power to rescind doctors’ medical licenses if they dissent from government positions on Covid, which are effectively dictated by Big Pharma.
To fight the malevolent forces behind these campaigns, we need to reform our dysfunctional drug approval process. Pierre’s outlines what needs to happen:
An independent board free of pharma industry conflicts must be established to oversee trials for re-purposed medicines. Recommendations should be based on trials designed by impartial experts and actual results, not the desired ones, and policymakers or prescribers who ignore the findings should be held accountable.
We must also remind academia and the regulatory agencies that observational trials data—wherein a sample of population who take a drug are compared to those who do not is equally valid at informing policy. Since Covid, regulators and academic medical centers have erroneously placed greater emphasis on large, expensive randomized controlled trials. While these trials can yield useful information, but their complexity, costs, and delays to treatment lead to errors and effectively shut out low-cost drugs from the approval process, regardless of their efficacy.
If our leaders in government fail to heed this advice, greed will continue to corrupt scientific study and erode the practice of medicine until doctors and patients are further relegated as little more than cogs in a billing machine.
You can read Pierre’s op-ed in full at The Brownstone Institute.
_________________
https://popularrationalism.substack.com/p/patient-attribution-bias-explains
Patient Attrition Bias Explains The Latest NEJM Ivermectin Study
Their data show the number of people who stayed 100% on protocol. Guess which group didn’t stay on protocol?
 |
This:

In double-blind RCT, ivermectin that was administered within 7 days after Covid-19 symptom onset was shown not to be of any clinical benefit. nej.md/3LtHLyh
Is not correct.
The study left out people who failed to adhere to the placebo treatment.
Check this out:
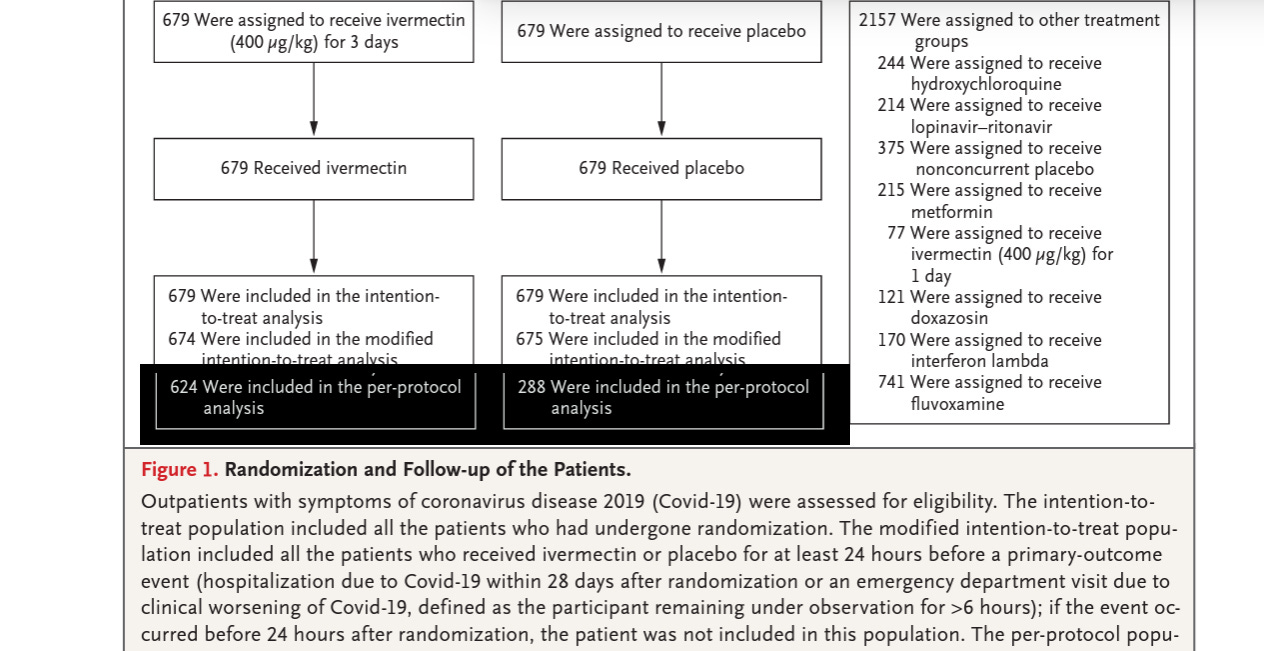
Both groups started with 679 people.
The Ivermectin group had 624 included after attrition.
For the per-protocol analysis, only 288 on placebo were still in the study.
Of the people who adhered to placebo with no benefit, we can expect they would have had more severe COVID-19 symptoms and sought treatment.
Note the patient attrition rate is far less in the Ivermectin group in the “100% Adherence to the assigned regime” analysis, but still biased toward people leaving the study to seek other treatment.
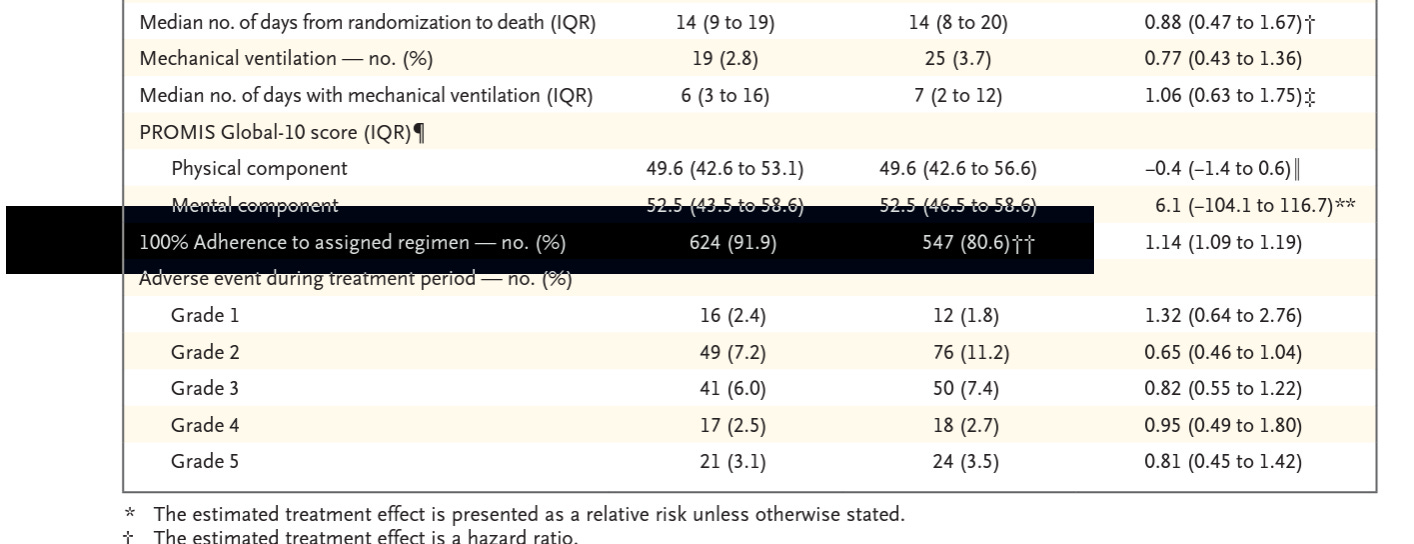
It’s a huge problem if more of one group is dropped from the study due to events that are clearly related to the outcomes measured.
The sickest people in the both groups would have started doing anything other than the pills they were given. The placebo group received visually identical pills in the identical packaging as the active drug, and they left in droves, whereas for the Ivermectin group, they clearly felt well enough to stay on the protocol.
Anyone can see that.
The paper is not to be taken seriously, and should be eliminated from future meta-analyses due to this obvious sign of bias.
__________________
Also see:
JAMA Ignores Peer-Reviewed Evidence & Publishes Yet Another Misleading, Underpowered IVM Study and WSJ & NY Times Mislead Public on New Ivermectin Study.
FLCCC Doctors: “We treat patients, not p-values.”
__________________
**Comment**
Dr. Kory’s outline of what needs to happen would also help those suffering in Lymeland as the very things affecting the ability to get effective COVID treatments are also affecking those with Lyme/MSIDS. We need a CDC/NIH/FDA walkaway movement.
Both of these studies serve as current reminders of the types of shenanigans that have been going on in Lymeland for over 40 years. Similarly to statistics, you can get research to say exactly what you want it to say by design.
In turn this rigged research has been used globally against patients, similarly to how extended antibiotic treatment has been denied Lyme/MSIDS patients due to study design. An example:
NY AG Letitia James’ “cease and desist” letters to doctors prescribing ivermectin are riddled with falsehoods.
Excerpt:
The “deceptive acts” to which the AG referred were outlined in the letter. (Note: All of the following noted by the AG are demonstrably FALSE, as evidenced by peer-reviewed science.)
FALSEHOOD #1: Providers of ivermectin are misleading consumers as to the effectiveness of ivermectin for COVID-19.
FACT: The effectiveness of ivermectin has been proven in over 70 scientific trials.
FALSEHOOD #2: Adverse effects associated with ivermectin are increasing, as shown in a rise in calls to poison control centers reporting overdoses and adverse effects.
FACT: After the New York Times reported that the Mississippi State Department of Health attributed 70% of its calls to ivermectin adverse events, they were forced to retract the figures. In fact, the ivermectin-related calls to the Mississippi State Department of Health represented only 2% of the total calls; and that 70% of those calls (1.4% of all calls) were from people who ingested veterinary grade ivermectin. (NOTE: The FLCCC has consistently advised against the use of animal-grade ivermectin.)
FALSEHOOD #3: The National Institutes of Health has determined that there is insufficient evidence to recommend ivermectin for COVID-19
FACT: The NIH has a “neutral” stance on IVM use.
The “deceptive acts” these doctors were accused of providing were, in actuality, courageous acts of life-saving compassion. Robust epidemiological studies from around the world validate the science in the real world and point to the effectiveness of preventive protocols based around ivermectin. But the well-coordinated and well-funded media campaign against ivermectin has strangled true science and caused the senseless deaths of hundreds of thousands.
For more:
