We really need to replace Kristen Honey and FAST. Given the information I have verified and documented, every day I am more concerned regarding how she claims to represent Lyme patient priorities. Nevertheless, she continues to play a central role in the Report process of the Tick-Borne Disease Working Group. This Report may have GLOBAL ADVERSE IMPACT on access to diagnosis and care.
Once you’ve had a chance to read the complaint, and if you agree the information contained makes Honey an unsuitable Vice-Chair for the Tick-Borne Disease Working Group, then …
…. please, AS SOON AS POSSIBLE, copy, cut and paste the complaint and mail it in (revisions are fine). The complaint is addressed to the person responsible for FACA, the Designated Federal Officer (DFO) of the Working Group and the alternate DFO.
I also ask that you share this GLOBALLY and ask others to TAKE ACTION.
Remember, we got rid of Wolitski! We can do this!
Thanks – Jenna
…………………………………………………………………………………………………
To: Tynetta.Dreher@hhs.gov, James.Berger@hhs.gov, Kaye.Hayes@hhs.gov
Cc: brett.giroir@hhs.gov
Subject: Failure to meet 21st Century Cures Act requirements and other Concerns
Dear Ms. Dreher, Mr. Beger and Ms. Hayes,
I have sound reasons to respectfully ask that Vice-Chair of the Tick-Borne Disease Working Group, Kristen Honey be immediately removed from her post:
1. apparently she has not truly represented a federal officer for the Working Group
2. while serving as Vice-Chair she is apparently seeking financing to bring a patent to market ‘to cure’ Lyme patients (and perhaps other patient groups)
3. her documented orientations toward healing has caused great concern among many in the Lyme community
I ask she be replaced with a federal officer familiar with complicated and persistent Lyme and coinfections, including tick-borne diseases and treatment options that have meet internationally accepted standards for clinical practice guidelines.
Not A Federal Officer
The Vice-Chair of the Working Group, Kristen Honey, is a Senior Research Scholar from Stanford University on assignment to the Office of Management and Budget, and apparently not a federal officer [1].
Her resume is on LinkedIn [2] and states from “January 2017 to present Senior Policy Analyst via Stanford University Interagency Personnel Agreement (IPA)”. The Intergovernmental Personnel Act (IPA) of 1970 allows the temporary assignment of skilled personnel between Federal and non-Federal entities.
However, since December 2017, Honey has been presented by HHS to the public as holding a White House post. Therefore, many of the those in the Lyme community assumed she was a federal official and met the criteria to be one of the seven federal voting members of the Working Group as required by law as required in the 21st Century Cures Act.
The SIX federal members are: 1. Charles Benjamin (Ben) Beard, 2. Commander Scott Cooper, 3. Dennis M. Dixon, 4. Captain Estella Jones, 5. Allen L. Richards and 6. Vanila M. Singh.
The EIGHT non-federal members are: 1. John N. Aucott, Chair, 2. Kristen Honey, Vice-Chair, 3. Wendy Adams, 4. Richard Horowitz, 5. Lise E. Nigrovic, 6. Robert Sabatino, 7. Patricia V. Smith and 8. Robert Smith
On June 16, 2018, during the Public Meeting of the Working Group I disclosed Honey’s legal status (in public comments) and now many in the Lyme community are disappointed to find that the Working Group leadership perpetuated what appears to be a deception regarding the Vice Chair’s federal status.
We also note that this failure to meet the basic membership requirements of the Working Group as cited in 21st Century Cures Act may invalidate all the Working Group’s efforts to date.
Fund Raising and Conflicts of Interest
Honey has a website that claims [4] (see under Kristen’s Journey) “… based on limited scientific information and guided by my own personal tolerance for the unknown and risk (and after six months of FDA-approved antibiotics/antifungals failing to work), I ultimately chose the unknown. I went outside the bounds of FDA-approved treatments and self-administer intravenous injections of nanominerals … Fortunately, the treatments worked … Today, after two and a half years (from 2009 to 2012)… I am symptom free and 100% Lyme free.”
(See under Book) “… the novel IV nano-mineral solution — which Dr. Honey pioneered and calls her “lynchpin” for Lyme recovery and thriving wellness — has been patented using open-source intellectual property (IP)…If you or your organization wish to support Dr. Honey’s vision to bring this IV nano-mineral solution to market through open-source IP and open-source medicine, we welcome contributions and collaborations [5].”
Apparently, while ‘appearing to be a federal officer’ on the Working Group, Honey’s website is also actively seeking funding to bring her non-FDA approved technology for Lyme patients to market and indicates it will cure the disease. This does not appear ethical.
Optics, Orientation and Related Concerns
The follow information has been widely disseminated in the Lyme community and generated much concern regarded Honey’s claims to represent patient interests and priorities.
Rachael Bleau [6] is a Doctor of Metaphysical Science. (Bleau’s Doctor degree can be earned on-line from the UniversityofMetaphysics.com.) Honey is featured in Bleau’s book titled Clear Your Way to Freedom —the key to unlocking your whole healing [7]. According to this book, Bleau uses a spiritual/religious belief in ‘Ascended Masters’ to heal persons [8].
Adherents of these Ascended Master Teachings, such as the Great White Brotherhood [9] believe that the All-Pervading Presence of God does not act nor create except through Its Individualizations. All creation comes forth through These Individual Identities and is sustained by Them. Included in this Cosmic Hierarchical scheme are Solar Logoi, Elohim, Sons and Daughters of God, Ascended Masters, Cosmic Beings, the Twelve Solar Hierarchies, Archangels, Angels, Beings of the Elements, and Twin Flames of the Alpha-Omega Polarity sponsoring Systems of Worlds and entire Galactic Systems.
Page 78 of this book describes Honey’s general background, confirming it is the same Kristen Honey who is the Vice Chair of the TBDWG [8]. According to this book, Bleau used her ‘spirit team’, which includes Ascended Masters, to heal Honey from illness including Lyme disease (page 76). On page 74, Bleau writes about finding an ‘unhappy attachment’ that was hooked on Honey’s left adrenal and ‘hanging on for dear life’. In this passage the author states she removed the unhappy attachment while Honey saw ‘black energy dissipating’. Bleau goes on to state that Honey then fills up with ‘a golden light like honey’ ‘just like her last name’.
On page 76, Bleau refers to the root energy of Honey’s debilitating Lyme disease as being evil. Bleau’s spiritual team was assembled and gave her instructions on where to place her hands on Honey. Bleau found ‘a dark seat of energy’ on Honey’s right thigh. Bleau then ‘profiled the energy’ to locate its home and claims to have heard a hissing sound, like that of a snake, when she pulled the evil energy from Honey’s body.
According to a 2013 blog by the Better Health Guy, Honey gave a presentation at the Integrative Lyme Solutions: The Evidence Basis Conference on June 21-22, 2013 in Dallas, Texas [10]. Honey shared her own personal recovery story. Honey spoke about how she was very sick, ‘likely from tick bites’ and struggled with Lyme infection, Babesia, Bartonella, Ehrlichia, and Mold. In her presentation, Honey noted:
× she did ‘mind, body and spirit work for her successful recovery’
× much of healing ‘is the responsibility of the patient to work on the spiritual or ‘upper levels’ of oneself
× her healing was supported by nanoparticles of gold and silver
Apparently, Honey said she ‘feels strongly that we [Lyme patients] can recover 100% if we choose to’.
Many in the Lyme community are concerned with Honey’s apparent orientation for healing from these complex diseases. Does she believe that persons suffering from Lyme disease, including chronic Lyme with serious debilitation and disability, choose to stay sick? Does this mean that Honey believes that these patients, many who are impoverished by their illness, should pay $350 for a 90 minute session with Bleau? Or someone with Bleau’s special healing powers? Or will patients be encouraged to purchase her ‘novel IV nano-mineral solution’ to be cured of Lyme?
Please remove Kristen Honey immediately from the post of Vice Chair of the Tick-Borne Disease Working Group, thank you.
YOUR NAME
…………………………………………………………………………………………….
Footnotes
[1] https://www.linkedin.com/in/kristenhoney/
[2] source: LinkedIn, CV on https://www.slideshare.net/slideshow/embed_code/key/gPTaDnPp1hyR6N
[3] https://www.hhs.gov/ash/advisory-committees/tickbornedisease/about/21-century-cures-act/index.html
[4] http://honey2healing.org/
[5] http://honey2healing.org/book/
[6] Rachael Bleau’s website https://www.rachaelbleau.net/
[7] Clear Your Way to Freedom by Rachael Bleau MSC.D. Copyright 2014 by Balboa Press. Please note this book has a disclaimer, “the author of this book does not dispense medical advice or prescribe the use of any technique as a form of treatment for physical, emotional, or medical problems without the advice of a physician, either directly or indirectly. The intent of the author is only to offer information of a general nature to help you in your quest for emotional and spiritual well-being”
[8] See pages 39,40,59, 61, 62, 76, 81 https://books.google.com/books?id=1sAAAwAAQBAJ&printsec=frontcover&dq=editions:vAGjiTCFQpAC&hl=en&sa=X&ved=0ahUKEwiE68Cs-OHaAhXvmuAKHbCCC7oQ6AEIKTAA#v=onepage&q=Kristen&f=false
[9] Great White Brotherhood – https://www.summitlighthouse.org/great-white-brotherhood/
[10] Disclaimer from the blog of Better Health Guy: “Nothing in this text is intended to serve as medical advice. All medical decisions should be made only with the guidance of your own personal medical authority. This information was taken as notes during the conference and may not represent the exact statements of the speakers. Errors and/or omissions may be present. If you have any corrections to the content listed below, please Contact Me. [Better Health Guy]”
_______________
**Comment**
First, I’ll bet if you interviewed every single person on the Working Group about their beliefs, you’d hear 100 different answers. Personally, I don’t care if someone “believes” the moon is made of cheese as long as they have the ability to weigh those “beliefs” and make productive decisions for really, really, sick people, despite personal preferences, beliefs, and experiences.
The only potential problem with Honey’s “beliefs” and personal experience is she may make the mistake of feeling her experience is the “right” one. If there’s one thing I’ve learned on this journey to hell and back is that it hits everyone so differently and therefore requires different answers. Long-term antibiotics DO work for some, and for some they do not. To rule them out for everyone; however, would be foolish just due to the fact some continue to have symptoms.
What is super concerning is another conflict of interest. Conflicts of interest got us into this mess and they keep rolling out like a barrel full of monkeys. This HAS TO END! Since Honey stands to make money on her patented “nano particle” treatment, she stands to gain by downplaying or eliminating long-term or IV antibiotics for Lyme/MSIDS.
If you have a conflict of interest, GET OFF THE WORKING GROUP. Period. If you stand to make money based on decisions the group makes – GET OFF THE GROUP.

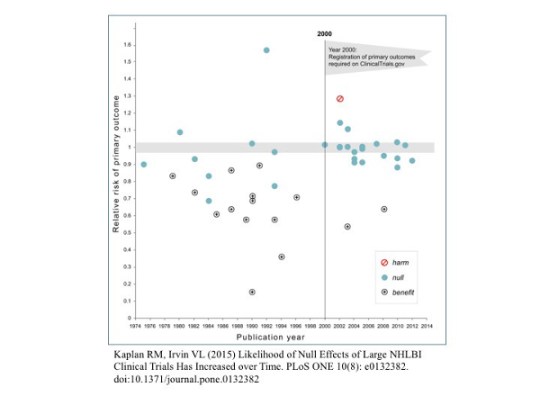 Rigging of Outcomes — Or consider the example of registration of primary outcomes. Prior to year 2000, companies doing trials did not need to declare what end points they measured. So they measure many different endpoints and simply figured out which one looked best and then declared the trial a success. Kind of like tossing a coin, looking at which one come up more, and saying that they were backing the winning side. If you measured enough outcomes, something was bound to come up positive.
Rigging of Outcomes — Or consider the example of registration of primary outcomes. Prior to year 2000, companies doing trials did not need to declare what end points they measured. So they measure many different endpoints and simply figured out which one looked best and then declared the trial a success. Kind of like tossing a coin, looking at which one come up more, and saying that they were backing the winning side. If you measured enough outcomes, something was bound to come up positive.