
Start Treatment if TBI’s are Suspected
http://www.mdedge.com/ccjm/article/141387/dermatology/tickborne-diseases-other-lyme-united-states Cleveland Clinic Journal of Medicine. 2017 July;84(7):555-567
KEY POINTS
- Tickborne illnesses should be considered in patients with known or potential tick exposure presenting with fever or vague constitutional symptoms in tick-endemic regions.
- Given that tick-bite history is commonly unknown, absence of a known tick bite does not exclude the diagnosis of a tick-borne illness.
- Starting empiric treatment is usually warranted before the diagnosis of tickborne illness is confirmed.
- Tick avoidance is the most effective measure for preventing tickborne infections.
____________________________________________________________________________
The article delineates symptoms, transmission, reservoirs, testing, and treatment of the following TBI’s: Rocky Mountain Spotted Fever, Rickettsiosis, Ehrlichioses, Babesiosis, Tickborne relapsing fever, Borrelia miyamotoi, Southern Tick-associated Rash illness, Tularemia, and Tickborne viral infections.
I need to address the following statements at the end of the article:
“Knowledge of the geographic locations of potential exposure is paramount to determining which tickborne infections to consider, and the absence of a tick bite history should not exclude the diagnosis in the correct clinical presentation.
Clinicians need to tread carefully here. Many patients have been denied testing and treatment due to a map. These maps should be viewed with the same suspicion as the testing.
Until you tell the fox, squirrel, bird, deer, lizards, and hundreds of other reservoirs to stay put, ticks will be traveling everywhere along with the pathogens they carry. Since Lyme Disease (borrelia) has been found in every continent except for Antarctia (it will be found there too), you can assume that means ticks are there too.
I’m glad the authors stated this:
In addition, it is important to recognize the limitations of diagnostic testing for many tickborne infections; empiric treatment is most often warranted before confirming the diagnosis.”
For those of us in this war, this “empiric treatment” by mainstream medicine is new. Patient after patient has had to wait for test results before doctors will treat them. Often, since the testing is so poor, it comes back negative and the patient is sent packing, even if the patient has every symptom in the book. The next step is for authorities to admit and acknowledge that diagnosis of Tick borne infections is a clinical one. This means doctors need to learn a whole lot more. For docs willing to learn, please see: https://www.lymecme.info
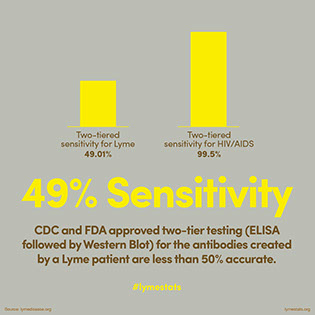
Even the CDC admits the tests suck: https://madisonarealymesupportgroup.com/2017/07/01/good-morning-america-cdc-advises-multiple-lyme-tests-due-to-false-negative-results/ CDC spokesperson at end of video.
Another very important point needs to be made. The CDC has pushed this one pathogen for one tick mantra for too long. Many patients are co-infected making cases infinitely more complex and challenging to treat. Lyme literate doctors trained by ILADS understand this and treat accordingly. Until mainstream medicine realizes and admits people can have numerous pathogens, and treat for them, people will not get better. This is why all the doxycycline in the world will not help some patients.
One last point is that mycoplasma, Bartonella, and other pathogens are not included here but are quite common in patients. Many of these pathogens are persistent and are adept at surviving. More research needs to be done on these co-infections.
Please see:
https://madisonarealymesupportgroup.com/2017/05/01/co-infection-of-ticks-the-rule-rather-than-the-exception/ If ticks are co-infected, so are patients.
https://madisonarealymesupportgroup.com/2016/03/20/why-we-cant-get-better/
