
New Maps Show Where Citizen Scientists Found Infected Ticks
https://www.lymedisease.org/balf-interactive-tick-maps/
New maps show where citizen scientists found infected ticks
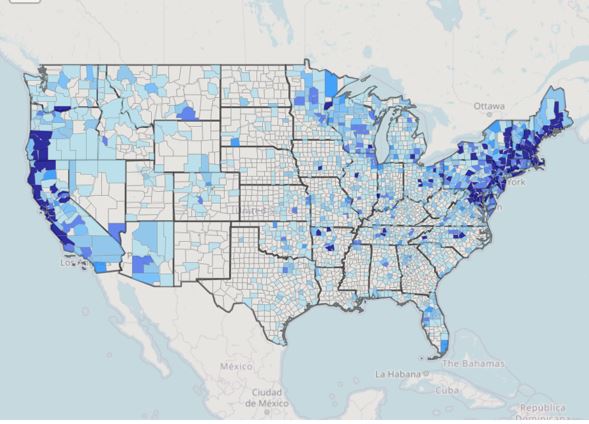
Want an easy way to see where disease-carrying ticks have been found throughout the United States?
Check out the new interactive tick maps recently launched by the Bay Area Lyme Foundation.
The maps are based on data published in mSphere, a multidisciplinary open-access journal of the American Society for Microbiology.
The information came from ticks submitted by citizen scientists as part of BALF’s Free Tick Testing Program, which ran from 2016 to 2019.
The study found infected Ixodes ticks in 116 counties which were not previously identified by the Centers for Disease Control as having them.
The testing program collected more than 20,400 ticks. 8,954 were Ixodes ticks, capable of carrying the most common tick-borne pathogens.
The research was conducted through a partnership between Bay Area Lyme Foundation, Northern Arizona University, Colorado State University and the Translational Genomics Research Institute (TGen).
The study evaluated the distribution and prevalence of the four most common tick–borne pathogens:
- Borrelia burgdorferi sensu lato, the group which causes Lyme disease
- Borrelia miyamotoi, which causes tick-borne relapsing fever
- Anaplasma phagocytophilum, which causes human granulocytic anaplasmosis
- protozoan pathogen, Babesia microti.
The program tested two types of ticks:
- Ixodes scapularis, also known as the blacklegged tick or the deer tick, which are found in the Northeast, Midwest and South;
- Ixodes pacificus, also known as the western blacklegged tick, which lives in the West
The interactive maps only represent data from this citizen science study. They do not represent the total risk of tick-borne infections in the US.
An eye-opening look
“These maps will be eye-opening for many Americans as it makes it easy to see that ticks carrying disease-causing bacteria can be commonly found across the US,” stated Tanner Porter, MS, a research associate at TGen and the lead author on the study.
“If you aren’t aware of the possibility of ticks, either in your backyard or whilst traveling, you are unlikely to look for them – but an unseen tick can still transmit a pathogen and cause disease. It is important for everyone to know to look for ticks, be aware of the pathogens that they carry, and takes steps to mitigate their risk.”
This new study expands on previous research identifying ticks capable of carrying Lyme and other tick-borne diseases in 83 counties (in 24 states) where these ticks had not been previously recorded. These included: Alabama, Arizona, Georgia, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Michigan, Minnesota, Montana, Missouri, Nevada, North Carolina, Ohio, Oregon, South Carolina, Tennessee, Texas, Utah, Virginia, Washington, and Wisconsin.
The study builds on recently released CDC data that added 100 counties to the list of those with disease-carrying ticks.
PRESS RELEASE SOURCE: Bay Area Lyme Foundation


