POSTED ON AUGUST 23, 2017
In this week’s issue of PEOPLE, former Real Housewives of Beverly Hills star Yolanda Hadid opens up about her battle with late-stage Lyme disease, and how the illness drove her to contemplate suicide. But what is the mysterious illness?
Lyme disease is a potentially debilitating infection caused by bacteria called Borrelia burgdorferi, and is transmitted through the bite of an infected blacklegged tick.
“For some people, Lyme is easily treated but for others this disease is devastating,” says Linda Giampa, executive director of the Bay Area Lyme Foundation. The CDC has also documented cases in which Lyme has been fatal. (See link for article)
For more on Hadid’s struggle with Lyme, check out her new memoir – Believe Me: My Battle with the Invisibility of Lyme Disease – which comes out Sept. 12.
Early in my career practicing Ob/Gyn, I became aware of a subset of patients who suffered from a condition called interstitial cystitis (IC), sometimes referred to as painful bladder syndrome.
People with interstitial cystitis feel like they have a bladder infection that never goes away. It doesn’t respond to antibiotics, and urine cultures are typically negative. Because these patients are often treated repeatedly with antibiotics, however, they frequently end up having chronic urinary tract infections with antibiotic-resistant bacteria induced by taking antibiotics. The condition occurs more often in women than men at a 5:1 ratio.
Interstitial cystitis is considered idiopathic — cause unknown. It is notoriously difficult to treat. I developed a special compassion for these people because no other physicians wanted to see them. For years, I searched for solutions, but my efforts were focused primarily on relieving symptoms — gains were minimal and short-lasting.
Symptoms of Interstitial Cystitis
Urinary frequency & urgency
Bladder pain with full bladder
Pain in perineum & urethra
Chronic pelvic pain
Vulvar/vaginal pain (female)
Pain in testicles (male)
Painful sex
The Lyme Connection
Interestingly, with my professional interests now focused on chronic Lyme disease, I’m starting to hear from chronic Lyme patients who suffer from bladder pain and symptoms consistent with IC. I’m also hearing from men with chronic Lyme who have bladder symptoms and chronic prostatitis (chronic infection of the prostate gland).
And, interestingly, remembering back to patients from the past, sufferers of IC frequently had chronic pain in other areas of the body. Many of them also had fatigue and symptoms common to fibromyalgia and chronic Lyme disease.
This makes me believe there has to be a microbial connection. Borrelia, the microbe commonly associated with Lyme disease, could be a culprit. However, I would lay odds on mycoplasma and a closely related bacterium called ureaplasma. About 75% of chronic Lyme disease sufferers have been found to harbor at least one species of mycoplasma.
It fits. Mycoplasma and ureaplasma are the smallest of all bacteria. They are obligate intracellular microbes — which means they must live inside cells of a host to survive. They typically infect linings of the body — linings of lungs, intestines, joints, and the urinary tract.
Different species of mycoplasma and ureaplasma prefer certain areas of the body, but any species of these microbes can be found in different places the body. The most common species found in the urinary and reproductive tract are Ureaplasma urealyticum and Mycoplasma hominis. These microbes typically spread sexually, but they can be acquired by other routes. Mycoplasma pneumoniae, a frequent cause of respiratory infections, can also be found in the urinary tract.
Mycoplasma and ureaplasma are notoriously difficult to culture. Twenty-five years ago, when I first started practicing medicine, routine testing for mycoplasma and ureaplasma was not available. That’s starting to change — DNA testing has become more reliable, and providers are testing for these microbes more routinely.
And they are finding them — not just in symptomatic patients, but also commonly in people with no symptoms.
That makes things complicated — mycoplasma and ureaplasma are commonly found in the urinary tracts of people who don’t have symptoms. It turns out that it’s actually a very common microbe. Some experts have even defined it as a normal flora. This is why many experts discount the connection between mycoplasma/ureaplasma and bladder problems.
It presents the same kind of conundrum found in chronic Lyme disease — why do some people with these microbes develop symptoms and others do not?
What I didn’t know 25 years ago that I learned from understanding chronic Lyme disease is that the immune system is the key. If people have robust immune function, they can harbor these microbes and not have symptoms. People become chronically ill only when a perfect storm of factors comes together to disrupt immune function, which allows the microbes to flourish.
Therefore the solution must go beyond killing or suppressing microbes — you must restore immune system functions to optimal levels to overcome this illness.
Overcoming Mycoplasma and Ureaplasma
Mycoplasma and ureaplasma respond poorly to synthetic antibiotics for the same reason that other microbes associated with chronic Lyme disease respond poorly to antibiotics — they live inside cells, grow very slowly, and occur in low concentrations in tissues. In addition, mycoplasma and ureaplasma do not have a typical cell wall and other characteristics common to bacteria.
To control them, you must suppress them for a very long time and boost immune function at the same time. If you try to do it with synthetic antibiotics, normal flora are disrupted long before the targeted microbes are eradicated.
Herbs provide a more practical solution. Herbs suppress these types of microbes, but do not disrupt normal flora, so they can be used for extended periods of time (months to years) without concern. Herbs also reduce inflammation and boost immune functions — especially natural killer cells important for eliminating cells infected with microbes.
My favorite herb for mycoplasma and ureaplasma in the urinary tract is anamu (Physalis angulata) because it is concentrated in the intestines and urinary tract. The dose I recommend is 1200 mg (2 – 600 mg capsules) twice daily. It is well tolerated with only noticeable side effect being a mild odor to urine and stool. The herb comes from South America, but is readily available from many manufacturers online.
Mullaca (Physalis angulata), another South American herb, is also good for mycoplasma species. It can be taken as a complement to amamu. It can be found online as a loose powder (add to smoothies or make your own capsules) or tincture, as well.
Stephen Buhner, in his book defining therapy for mycoplasma, recommends Chinese skullcap, Isatis, Houttuynia, Sida acuta, and Cordyceps for a primary herbal protocol. I consider Cordyceps and Chinese skullcap to be part of a core protocol for chronic Lyme in general.
Individuals are reporting symptomatic relief of IC symptoms with use of essential oils rubbed into the pubic area several times a day. I have been recommending a formula of tea tree oil and frankincense oil mixed 1:4 in a carrier oil, such as jojoba or grapeseed oil. Recently, I’ve also been recommending adding cannabidiol oil (CBD) from hemp (get a product with 1500 mg CBD per fluid oz.). So far, people are reporting positive benefits.
The recovery protocol for overcoming mycoplasma and ureaplasma in the urinary tract mirrors recovery from chronic Lyme disease or any other condition associated with chronic immune dysfunction. Focusing on a specific microbe alone is not enough; immune system function must be restored. Primary antimicrobial herbs and immune modulating herbs, complemented by cultivation of a healing environment within the body, are your best allies in the fight against interstitial cystitis and Lyme disease.
Dr. Rawls is a physician who overcame Lyme disease through natural herbal therapy. You can learn more about Lyme disease and recovery in Dr. Rawls’ new best selling book, Unlocking Lyme. You can also learn about Dr. Rawls’ personal journey in overcoming Lyme disease and fibromyalgia in his popular blog post, My Chronic Lyme Journey.
_______________________
**Comment**
Wonderful article. Thank you Dr. Rawls for explaining a particularly troubling issue that Lyme/MSIDS patients can suffer from.
“….90% of evaluated ALS patients had Mycoplasma. 100% of ALS patients with Gulf War Syndrome had Mycoplasma and nearly all of those were specifically the weaponized M. fermentans incognitus. *One of the hallmark symptoms of Mycoplasma is fatigue* And the bad news for us is that Nicholson’s experience has found Mycoplasma to be the number one Lyme coinfection, and similar to other coinfections can be supposedly cleared for years only to reappear when conditions are right.”
The evidence from the study reveals that MTP (Myofascial Therapy) is indeed beneficial for improving symptoms of IC, suggesting that physical therapy is an important modality to consider in a treatment plan for a patient suffering from the disease. It adds credibility to the idea that there are specific pelvic somatic abnormalities involved with IC, as the study showed the treatment effect was not merely due to general therapeutic touch.
Infections with tick-transmitted Borreliella (Borrelia) burgdorferi, the cause of Lyme disease, represent an increasingly large public health problem in North America and Europe. The ability of these spirochetes to maintain themselves for extended periods of time in their tick vectors and vertebrate reservoirs is crucial for continuance of the enzootic cycle as well as for the increasing exposure of humans to them. The stringent response mediated by the alarmone (p)ppGpp has been determined to be a master regulator in B. burgdorferi. It modulates the expression of identified and unidentified open reading frames needed to deal with and overcome the many nutritional stresses and other challenges faced by the spirochete in ticks and animal reservoirs. The metabolic and morphologic changes resulting from activation of the stringent response in B. burgdorferi may also be involved in the recently described non-genetic phenotypic phenomenon of tolerance to otherwise lethal doses of antimicrobials and to other antimicrobial activities. It may thus constitute a linchpin in multiple aspects of infections with Lyme disease borrelia, providing a link between the micro-ecological challenges of its enzootic life-cycle and long-term residence in the tissues of its animal reservoirs, with the evolutionary side-effect of potential persistence in incidental human hosts.
—————————————————————————————————————————————–
**Comment**
The idea of sleeper/persistent cells in Lyme and other TBI’s is nothing new to those actively treating patients. It’s just a matter of time before enough people in power positions acknowledge it. Also, it needs to be understood that those infected with Lyme often have numerous pathogens that don’t respond well to the mono therapy of Doxycycline and is one reason outcomes are not good.
BVIKZ interview The sound of the movie is softer than intended, so it is subtitled in both English and Dutch. Click on settings to select your language.
The BVIKZ, the Interest Group for Intensive Child Care, is doing an ongoing investigation into false claims of child neglect and abuse by the Dutch Child Protection Services. It has now compiled and researched 168 individual cases. Over thirty percent of these cases are about children with Lyme disease.
During the last eight months hundreds of Dutch parents have been contacting the BVIKZ to report what happened to them. They have also received many reports from parents of children with Lyme disease. National media made this into a primetime topic, which was viewed by 1.5 million people. Shortly afterwards the BVIKZ had their third meeting with the Board of the Dutch Child Protection Services called ‘Safe Home’ (SH).
BVIZK chairman Vera Hooglugt agreed to do an exclusive interview for the On Lyme Foundation. We asked her to tell about their general findings of the BVIKZ investigation and specifically about the Lyme cases. The interview took us over three hours.
The BVIKZ has been working intensively to build all cases, scan all files, support the traumatised parents and children, assist in conversations, provide legal help and build up a case to create political impact to fundamentally change the way the whole system is operating. The meetings with SH are absolutely very important for the process.
Hooglugt thinks that they are only just seeing the tip of a much larger iceberg and wants to encourage other parents to be brave and come with their complaints in case of false allegations.
The tipping process
Tips or reporting seem to come from all angles. Tips come from all angles and we have the impression that the ones doing the reporting don’t realise how much impact it can have on the lives of the children and the families.
Almost all of the reports we saw are subjective and most are very suggestive. As an independent organisation we can really be neutral and unbiased enough to look at the claims without prejudice. So we strip all assumptions, subjective ‘gut feelings’ and also check on the motives of the ones doing the reporting.
Too often we see that the child’s best interests in not at stake. We often see divorced husbands reporting on their ex-wives. The system just regards this as an objective fact, worthy of a formal investigation.
Another example is a government official charged with school absence, who had already given the child leave to skip school. When the family moved house, he found what province they had moved to and asked his colleague to assist in filing in a report on ‘child abuse’.
In another case a commercial company was annoyed that they did not get a contract, because the parents did not find the care provided as fitting for their child. The company reported on the parents and SH did a year long investigation, wrecking the social life of this family.
We urged the parents to ask for the original report, which is within their rights. Their request was denied without reason, so we filed a request as their formal representative.
We then received a paper copy, in which a large part of the text was white-washed. Again we requested the original digital version from SH, but were told that it was deleted due to computer problems. Finally we managed to get the original complaint. By comparing the different versions we could see that all subjective remarks were white-washed.
Employees of the Consultation Office, where new parents go to check on their baby’s health and progress, have been reporting them to SH. Simply for not vaccinating their child or wanting to use other services offered by this institution.
Another poignant case is the one of an adult lady, who suffers from Lyme Disease and who is been taken care of by her old mother. She cannot stand light or sound, so she lives in a darkened room. The mother of a distant acquaintance of their neighbour reported on them, after hearing a gossip story about closed curtains. People like her seem to be influenced by prompting calls in the media.
In this case SH tried to get a psychiatrist to both judge the mother with ‘Munchausen by Proxy’ and proclaim the daughter legally ‘incompetent’ (not having her own will). This would allow them to lock her up in a psychiatric ward and blame the mother. Why would Youth Care deal with someone who is of age? After a change in Dutch policy they now have the function to provide safety in everyone’s life; from zero to hundred.
Although these examples are shocking enough in themselves, we also saw statements of how family doctors state that they were intimidated by SH to testify against their patients. Fortunately they refused to act against their Hippocratic Oath to ‘first not do harm’.”
The foundation of the accusations
In all cases we see how easy it has been made for anyone to report on everyone else. This allows everyone to report, without a proper filter in the system. Even though a ‘code of conduct’ has to be used, we see that happening far too little. Although Dutch Law obliges SH to do ‘truth finding’ or objective research, we don’t see this is organised well enough by the different organsiations involved in this field. Our conclusion is that a legal perspective needs to be added: are there enough facts present to merit an investigation.
SH does work with the ‘Triage Model’, but if you look into it, you see meaningless categories and no expertise to actually judge them. The overall tendency is that the people working at SH are committed to ‘win the game’, no matter what. In our investigation we do a scan on who is doing the reporting.
We have compiled a spreadsheet of what is being used as the basis for the allegations. Concerns for ‘social isolation’, ‘cognitive well-being’, ‘somatic well-being’, ‘emotional well-being’. Not going to school for a few weeks is considered as damaging the ‘cognitive well-being’ of the child and thus framed as ‘child abuse’.
So these definitions used in this Triage model are so broad that any report, no matter how suggestive, automatically leads to a formal investigation. The fact that a child has not been to school for several weeks, is framed as ‘damage to mental mental health’ and later as child abuse.
If you look at how these organisations build their cases, these ‘investigations’ serve one purpose only: to get their way. The result is forced measures that are imposed on the family. In Dutch these are either called OTS (state surveillance) or UHP (placement in a foster home).
From all the files we have studied, the fosters from almost all these organisations are disastrous for the children. In a case of a girl with Lyme the foster told her that she was faking the disease and that since his contract said he should force her to go the school, that was what he would do. The girl fell asleep within one hour in class out of pure misery.
Reversed proof
Oftentimes we help parents in these cases. From this experience and the 168 cases we have already investigated, we see that SH operates from a predisposed distrust. They are backed up in this attitude by the organizations that are supposed to provide an objective and unbiased check.
Parents are charged under Criminal Law (articles 300 – 304 in Dutch criminal law). What shocked us is that they are forced to cooperate towards their own conviction. In essence this means that parents are convicted upfront, unless they can proof they are innocent, which is hard to do, given the amount of stereotyping. (attorney Richard Korver, who was recently interviewed in Dutch to provide practical information to parents with children with Lyme, suggested that the legal prinpicple of Confidence be used more often. This means to start with the assumption of attitude that most people simply care for their children; unless proven otherwise.)
Often on the same day a child is released, we see SH apply for a fast track procedure in court. Without the needed for any further research, custody is taken away, based solely on the claim that there is ’eminent danger in the home situation’.
Different organizations are supposed to act as an impartial factor, but we basically see copying and pasting. SH copies the subjective tips and frames them into legal language. The Council for Child Protection (RvdK) copies these reports in their independent evaluation. Judges copy these conclusions in their verdicts. The other side is not even heard.
The Lyme cases
“We have now researched over fifty cases; the ones which we have fully assembled. These people came after the On Lyme Foundation and the Dutch Federation for Lyme Patients (NVLP) notified them to our research. We had no idea Lyme was such a problem because of the medical and political controversies around it.
We have the strong impression that there are many more Lyme parents, who have become victim of SH but who do not yet dare to contact us. Some parents are so traumatized, it takes us ten phone calls to reassure them that their information is really save with us.
We do see some specific differences with other diseases, which have a less disputed status. Apparently national Lyme policies dictate that after a few weeks of treatment, the cause of the disease is suddenly a ‘mental issue’ (called MUS: Medically Unexplained Symptoms). Regardless of the fact that these children are still as ill as before.
Again and again we hear stories of parents who tried everything to get medical help in the Netherlands, but who had to go abroad to find better help. The SH doctors overrule the decisions of these specialised physicians instead of cooperating with them.
Suggestions to remedy the system
Some political parties have started to get interested now; however, what they propose is by far not enough to put a stop to this.
If our investigation of these 168 cases is any indication of the general tendency of how the whole chain of Youth Care acts, we are facing a very grave problem. Every day new cases come in and we cannot even keep up with it, since we want to research it meticulously.
In short our recommendations would be:
Awareness of the ones doing the reporting & how much impact it can have
A better check on the validity of the reports, before the start of a formal investigation
Create an independent supervisory system with a Disciplinary Board
Stop SH doctors from questioning or interfering with medical care without consulting with the parents and other specialists
Judges should have their own check instead of relying on the reports of this system
Stop the liberty of SH to order a fast track judgement, with no need for any investigation
Provide money for aftercare of the victims, but certainly not by SH itself
Have the Inspection perform an investigation into how SH operates
Looking at the stacks of paperwork on their table, BVIKZ concludes: “This is the actual child abuse”.
A call to parents
The BVIKZ has to limit its investigation to the Netherlands and can hardly deal with the number of complaints now. Still, they encourage Dutch parents to file their complaints with them, so that together they can make a difference and stop the system from traumatising families like this. You can report them by email.
The On Lyme Foundation however would like to get an impression of the number of parents who faced similar situations in other countries. If you are not from the Netherlands, but you had similar experience because your children suffered from Lyme or its many misdiagnoses, you can mail us (also confidentially, of course) with a short description of what happened.
Note from the interviewer
This topic ties into what is recently discovered regarding the role of the World Health Organization (WHO) regarding the international diagnostic codes for Lyme disease. The WHO has not properly updated their ICD-codes to reflect the many conditions caused by Lyme borreliosis.
These outdated codes contribute to children being classified as having ‘non-specific’ illnesses and having treatments that are ‘experimental’. This allows for the allegations towards both parents and their ill children as well as their expert physicians.
Similar abuses can befall anyone, but is it particularly problematic for those who are already vulnerable. The outdated codes contribute to discrimination and marginalization by many institutions against this patient group.
This topic has hardly even been broached here in the U.S., but abuse allegations are happening regularly to families with Lyme/MSIDS. This is why I support the Parental Rights Amendment so parents are not forced to comply with the arbitrary U.N. Rights of the Child which effectively imposes international law upon families which is NOT in the best interest of children. For more: https://madisonarealymesupportgroup.com/2017/04/20/why-we-need-the-parental-rights-amendment/
https://madisonarealymesupportgroup.com/2017/05/18/first-peer-reviewed-study-of-vaccinated-vs-unvaccinated-children/ For families struggling with Lyme Disease, they are already fighting a system that doesn’t know how to cope with very ill children who often can’t keep up. Their little bodies are in a raging war of epic proportions. They are often bullied and mocked not only by peers but even by teachers and standard medical professionals who believe they are just being lazy. Infected, exhausted parents often don’t have the energy to fight the “mandatory vaccine” regimens being pushed upon them so just go along rather than weighing in their child’s current health issues. The entire system is stacked against them – forcing many to homeschool just to avoid the unbelievable pressure to conform.
LYMEPOLICYWONK: Canine maps predict Lyme disease risk better than the CDC does.
Dogs are considered a good gauge of the exposure of their human owners to infected ticks because they usually share the same environment and visit the same outdoor areas. In other words, canines are considered to be sentinel indicators of Lyme disease risk for humans. Not all dogs who test positive for Lyme antibodies are ill. However, they have been exposed to the Lyme disease bacteria.
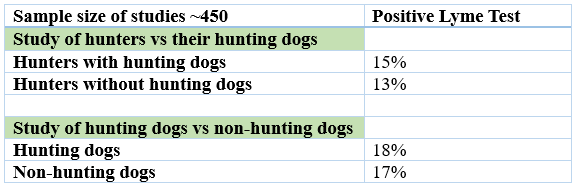
A combination of studies out of the Netherlands found that hunters and their hunting dogs had tested positive for Lyme disease at similar rates (17% hunting dogs vs. 15% hunters.)
However, the same study found that pet ownership itself did not increase risk, but that exposure was the primary factor: “Only 12% of the seropositive hunters had hunting dogs which were also seropositive. Moreover, hunters without dog ownership showed no significantly lower rates of seropositivity.”
Unlike people, dogs are routinely screened for Lyme disease and other common co-infections by their vets. IDEXX has tracked Lyme disease and other tick-borne diseases in canines for years by collecting data from veterinarians who test dogs at annual check-ups.
Between 2011 and 2015, IDEXX collected nearly 12 million Lyme disease test results from US veterinarians on a county-by-county basis. The data indicates that Lyme disease is present in abundance in every state in the US.
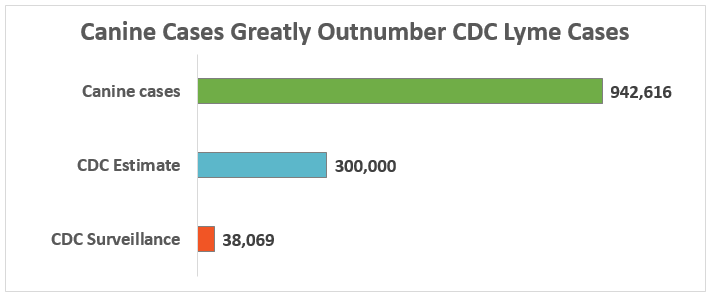
The number of canine positive test reports is vastly greater than the number of human cases reported by the Centers for Disease Control (CDC). There are close to one million canine positive test results annually in the US, compared to 38,069 cases included in CDC surveillance reports.
This means that there are roughly 25 times more canine cases than CDC surveillance cases. Even taking into account the fact that the CDC acknowledges that surveillance reports significantly underestimate the real incidence of Lyme disease by a factor of 10, the discrepancy is extraordinary. As the chart below reflects, canine cases are still more than three times the number of CDC estimated cases (300,000).
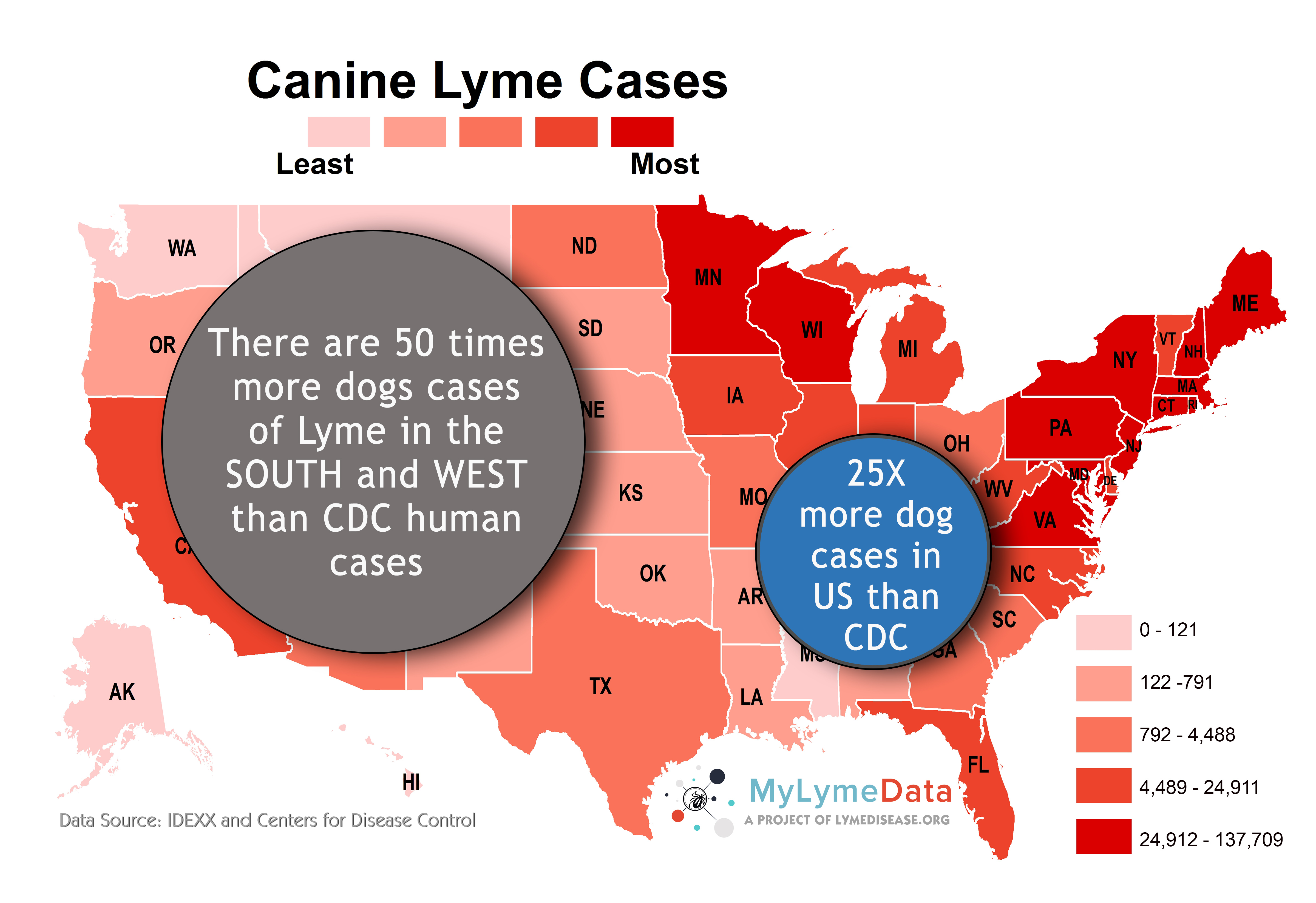
The discrepancy between CDC and canine cases is even more pronounced in the western and southern states. In the West and the South, there are 104,104 cases in dogs annually, compared to 2,342 CDC-reported cases. In other words, there are roughly 50 times more canine cases than CDC surveillance cases.
Michael Yabsley, a parasitologist at the University of Georgia, and Christopher McMahan, an assistant professor of mathematical sciences at Clemson University, have used the IDEXX canine data to develop a risk forecast map for the predicted Lyme disease prevalence — the percentage of dogs who are likely to test positive — by county in each of the 48 contiguous states. Yabsley explains the predictive relationship:
“Dogs really are the canary in the coal mine for human infection. Our research team has evidence that the relationship between canine disease and human disease is strong. Because dogs are being tested for exposure during annual exams, these data are available on a national scale, something that is difficult to get when studying the ticks and environment directly.”
Aside from indicating environmental exposure risk, the data illustrates that people who own pets need to be aware that they face the same exposure when walking their animals or when their animals return home from outdoors carrying ticks. Hence, preventative measures for pets—such as using appropriate tick and flea collars—are essential health matters for both people and their pets to avoid exposure.
LymeDisease.org believes that the IDEXX maps, which track Lyme disease as well as other tick-borne diseases such as ehrlichiosis and anaplasmosis, are the most accurate reflection of exposure. You can type in your zip code in the top right corner to assess your riskhere.
For example, in my zip code alone in Los Angeles, 626 cases of canine Lyme disease have been identified. (There are more than 3,500 zip codes in Los Angeles county.) That’s substantially more than the CDC reports for Californiaas a STATE for the last five years (2010-2015).
If you are interested in more information, check out the LymeSci blog on the predictive mapping of canine risk.
The LYME POLICY WONK blog is written by Lorraine Johnson, JD, MBA, who is the Chief Executive Officer of LymeDisease.org. You can contact her at lbjohnson@lymedisease.org. On Twitter, follow her @lymepolicywonk. If you have not signed up for our patient-centered big data project, MyLymeData, please register now.
**Comment**
Fantastic, informative article and so true. My dog got better treatment than we did. The tests for animals are much more accurate and veterinarians completely understand the seriousness of TBI’s (tick borne illness) unlike human doctors. Our vet had NO TROUBLE treating my dog for over a month even though HE HAD NO SYMPTOMS. Compare that attitude with the reality of multitudes of humans being continually turned away because of arbitrary reasons such as a lack of an EM rash, a map that demonstrating a lack of ticks or infected ticks on that geographical region, not enough time passed before accepted dogma of transmission, and so many other reasons.