The Defender is experiencing censorship on many social channels. Be sure to stay in touch with the news that matters by subscribing to our top news of the day. It’s free.
EDITOR’S NOTE: As The Defender reported this morning, U.S. health officials paused vaccinations with the Johnson & Johnson vaccine following multiple reports of people who developed blood clots after receiving the vaccine. Health officials said the pause is immediate but temporary. The article below was written before J&J vaccinations were paused.
Everyone is talking about DNA/RNA vaccines. Can they alter our own genetic codes?
The vaccine lobby says “Never!” I, however — laboring beneath the weight of a Ph.D. in virology — would instead quote Gilbert and Sullivan: “Well, hardly ever.”
Most people don’t know very much about DNA or RNA, so I’ll start with a 30-second chemistry discussion. DNA and RNA are both polymers, long strings (in this case, very long strings) composed of seemingly endless repetitions of a single basic chemical building block, called a nucleotide.
The resulting structure is often likened to a string of pearls, or to the rungs of a very, very long ladder. A single human cell contains some 6 billion nucleotide building blocks in its chromosomes.
In the picture below, the DNA basic building block is on the left, and the RNA building block is on the right. Take a look and see whether or not you can discern the difference:
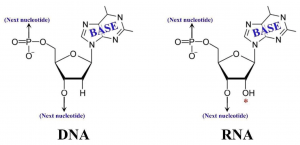
Don’t see much difference? That’s because there isn’t much. The red asterisk (*) shows the primary difference. RNA has an extra “O” (the abbreviation for an Oxygen atom). That’s about it.
Viruses have no lives of their own. They can grow only in host cells, such as, for example, your cells. In order for a virus to infect you, it needs to recognize a “receptor” on your cell surfaces. If — and only if — the virus can recognize such a receptor, then it has its own clever way of attaching itself to that receptor and sneaking its DNA (or RNA — viruses can have either one) into your cells.
Once inside, the DNA (or RNA) virus chromosome proceeds to reproduce itself, giving rise to hundreds or thousands of exact copies. These are then turned into complete virus particles by being covered with a protective protein coat. Next, the cell is broken open and the new progeny viruses disperse, infecting hundreds or thousands of other cells.
It’s easy to see how a viral infection can spread like wildfire in your body.
Even though the chemical differences between DNA and RNA are relatively small, the cell is smart enough to instantly recognize those small differences and act accordingly.
DNA is replicated in our cells by means of an enzyme called “DNA polymerase.” RNA, however, will not ordinarily be replicated by our cells because that’s simply not the way things work. So how does the RNA virus reproduce?
Some RNA viruses have an enzyme called “reverse transcriptase,” which begins each new viral life cycle by converting the virus’ RNA chromosome into DNA. This DNA copy can then be replicated by the cell’s own DNA polymerase-based system.
But other RNA viruses, including the COVID-19 strain of coronavirus, bring in their own special reproductive enzyme called “RNA polymerase,” which has the ability to directly produce numerous copies of the virus’ own RNA chromosome without any help from the cell’s native DNA polymerase system.
Now let’s speak for a moment about alteration of our genetic code. The interaction between a virus and the host cell is generally classified as being one of two distinct types of interaction.
Historically, the first type of interaction (discovered in the late 19th and early 20th centuries) was what we now call, in retrospect, a “productive infection.” Here the virus reproduces and kills the cell, releasing the many progeny as described above.
It was only in the later years of the 20th century that it became clear that there is a second sort of interaction, very different in nature, known as a “transforming” interaction (also called a “latent” infection). In a transforming interaction there is no virus growth at all. Instead, the single chromosome of the virus uses its bag of genetic tricks to insert itself into one of the 46 chromosomes of the host cell. There the viral DNA remains, sometimes forever.
In some species, such as herpesviruses, the virus’ chromosome just sits there, inside the host chromosome, apparently doing nothing — unless and until some sort of stimulus causes it to “pop out” again and begin growing. This produces a “cold sore” of the lips (herpesvirus type 1) or genitalia (herpesvirus type 2).
A large number of publications have documented that many — perhaps most — human beings have, within their nervous systems, cells which quietly harbor latent herpesvirus infections, even though the majority of humans will never get a cold sore. It is a known fact that herpes type I, in the latent state, resides in the trigeminal ganglion, inside the skull near the spinal cord. It is believed to be perfectly harmless in this latent state.
Other viruses, however, are not harmless in the latent state. A good example is SV-40, a DNA virus which is known to be capable of causing cancer in many mammalian species. SV-40 infects cells, but it usually doesn’t grow. Instead, it inserts its own chromosome into one of the cell’s chromosomes (a process called “integration”), and from that new base of operations it converts the cell from a normal cell, which is subject to normal forms of growth control, to a malignant cell which respects none of the host organism’s growth controls, and thereby causes cancer. This alteration, from normal to cancerous, is referred to as a “malignant transformation.”
But the term “transformation” does not automatically connote malignancy. Although a “transformation” may be harmful in any number of ways (and not solely limited to cancer), it might in other cases be entirely inconsequential (as far as the eye can see). In special cases, it might even be beneficial.
Curiously, however, even now — 68 years after the publication of the “Watson-Crick double-helix” structure for DNA — the dream of curing disease via human genetic re-engineering, employing custom-made viruses, remains in its infancy.
On the other hand, certain questionable forms of hastily-contrived human genetic experimentation, empowered by “executive orders,” and facilitated by “fast-track” bypassing of safety protocols, have become alarmingly commonplace.
Can a DNA-based vaccine ‘transform’ a human cell into something genetically different?
With all this in mind, we can now ask the question of whether or not a DNA-based vaccine might “transform” a human cell into something genetically different.
This is no small question, because if the answer is “yes,” and if the transformation proves to be harmful, then that harm may be passed to every subsequent generation — forever.
From 1972-1978, I was an M.D. – Ph.D. student at the New York University School of Medicine. Our lab addressed a question which was current at that time: In “productive infections,” where a virus replicates in cells and ultimately destroys them, might there nevertheless be integration of viral DNA into the host cell chromosomes?
We asked that question because, at that time in virological history, it had become abundantly clear that many different types of viruses could transform many different types of cells into malignant cancer cells. Those cells, if transplanted into animal hosts, would then form cancerous growths which would quickly kill the animal.
This sort of virus-mediated malignant transformation always began with the insertion (i.e., integration) of viral DNA into the chromosomes of the host cells. (Yes, I’m talking about that which the vaccine companies “assure” us will not follow vaccination with their “fast-tracked” new products).
Once these viral genes take up residence in host cell chromosomes, they are thereby empowered to seize control of the cell’s metabolism, perverting it to their own purposes.
So the question virologists were asking in the 1970s was this: Is the insertion of viral genes into host cell chromosomes a process uniquely associated with cancerous transformations? Or might the insertion of viral genes into host cell chromosomes take place in any and every sort of viral infection, whether it was a “productive” infection leading to virus multiplication and cell death, or whether it was a “transforming” infection where there was no virus multiplication at all?
We looked into this question by studying the infection of mammalian cells by herpesviruses. In the end, we published three papers, all in leading virology journals. These papers, listed below, are very difficult reading for anyone not familiar with the peculiar jargon of the field. But for those who are interested, here are the three references:
- Rush MJ & Biegeleisen K. Association of Herpes simplex virus DNA with host chromosomal DNA during productive infection. Virology, 69:246-257 (1976). https://doi.org/10.1016/0042-6822(76)90211-7.
- Rush MJ, Yanagi K & Biegeleisen K. Further studies on the association of Herpes simplex virus DNA and host DNA during productive infection. Virology, 83:221-225 (1977). DOI: 10.1016/0042-6822(77)90227-6.
- Yanagi K; Rush MG; Biegeleisen K. Integration of herpes simplex virus type 1 DNA into the DNA of growth-arrested BHK-21 cells. Journal Of General Virology, 44(3):657-667 (1979). DOI: 10.1099/0022-1317-44-3-657.
The first paper proved that herpesvirus genes are integrated into host cell chromosomes, but left some important questions unanswered concerning the physico-chemical nature of the linkage between viral and host DNA.
By the third paper, however, all reasonable doubt about the integration of viral DNA into host chromosomes had been laid to rest.
Another line of investigation going on at about the same time, in the laboratory of W. Munyon, led to the same conclusion. Munyon and his associates studied an enzyme called “thymidine kinase.” What that enzyme does is extraneous to this discussion. What matters is that the gene for the enzyme is normally found in human chromosomes, and also in herpesvirus chromosomes.
Munyon and his team had a mutant strain of cells that lacked the thymidine kinase gene. They infected those cells with herpesvirus that had been irradiated, and thereby rendered incapable of multiplying in and killing the cells.
But the virus did, nevertheless, carry in its own thymidine kinase gene. Upon infection, the cells were shown to suddenly have acquired that enzyme, even though they were mutants who had none of their own. Because the virus had been irradiated, it did not kill the cells, which continued growing in the laboratory.
Eight months — which is hundreds of generations — later, the progeny of those cells were still producing thymidine kinase!
So if a DNA vaccine company alleges that their vaccine will cause my cells to temporarily manufacture corona spike protein, but will not permanently “transform” my cells in any other way, what am I to think?
Or, perhaps I’m not supposed to think?
So far we’ve talked only about herpesvirus. The new Johnson & Johnson vaccine uses “reproductively incompetent” genetically engineered adenovirus as the carrier for the corona spike protein gene.
Should we worry? After all, unexpected integration of viral genes may be peculiar only to herpesvirus, and not adenovirus, right?
Unfortunately, that’s not the case. What I did not realize, at the time I was doing my own Ph.D. research on herpesvirus, was that other labs were conducting the same type of research on the adenovirus. Here’s an example of that work:
Schick J, Baczko K, Fanning E, Groneberg J, Burgert H, & Doerfler W (1975). Intracellular forms of adenovirus DNA: Integrated form of Adenovirus DNA appears early in productive infection. Proc Nat Acad Sci USA, 73(4):1043-1047. DOI: 10.1073/pnas.73.4.1043. PMID: 1063388. PMCID: PMC430196.
Like coronavirus, there are dozens of known adenovirus types, most of which are classified as “cold viruses.” But some adenoviruses cause much more serious disease, including cancer.
In the 1970s, the adenovirus researchers were asking the same questions that the herpesvirus workers were asking. And they were coming up with the same answers: In “productive infection,” where adenovirus was supposed to only replicate and destroy the cell, there was indeed extensive integration of viral genes into the host cell chromosomes — even though there was no obvious biological reason for the virus to do that.
No guarantees, despite what vaccine makers say
It seems that in many, perhaps most viral infections, integration of viral DNA into the host cells is a very real possibility. When this occurs, there is absolutely no way to “guarantee” that the genetic code of the host cell will not be re-written.
The question then arises: If this is the case, why do vaccine manufacturers “assure” us that their marginally tested products are genetically “safe?”
I would suggest three possible explanations, all equally reprehensible:
- It may be that the scientists in these companies simply do not know the history of this field. What can one say? “Those that fail to learn from history are doomed to repeat it.”
- It may be that anything in industry which does not improve the quarterly profit report is at great risk of being ignored.
- It may be that calling a new vaccine “safe,” in the pharmaceutical world, means little more than that the company has the legal resources to deal with any liability claims that arise.
Which of these three possible explanations is the correct one? Or is it all three?
In any event, you now know why I shall not take the Johnson & Johnson vaccine.
What about RNA vaccines?
We’ve been discussing DNA vaccines. What about RNA vaccines, such as Pfizer and Moderna?
Although I have no personal experience working in the lab on genetic transformation of human cells by RNA viruses, it is appropriate to comment briefly on that subject before closing.
The RNA vaccines are alleged by their promoters to be genetically “safe” because RNA cannot be directly incorporated into human chromosomes.
Is that true? Yes. But does that make them “safe?” Perhaps not.
What the vaccine companies forgot to tell you is that our cells have several types of “reverse transcriptase” of their own, which can potentially convert the vaccine RNA into DNA.
In December 2020, a team of researchers from Harvard and MIT (Zhang et al) posted an article at the Cold Spring Harbor Laboratory-hosted bioRxiv preprint server showing that, in all probability, incorporation of coronavirus spike protein genes, into the chromosomes of infected cells, does indeed take place, and is mediated by the so-called “LINE-1” type of human reverse transcriptase. (For more on the Harvard-MIT study and its implications, read this article previously published by The Defender).
To be clear, this was not a vaccine study, but a study in which cells were deliberately infected with whole, non-inactivated virus, as happens in nature, and which apparently can result in genetic transformation of the cells after all.
This, suggested the authors, may account for the now-frequent observation of COVID-19 test “positivity” in people who are clearly not sick. That is, the bodies of such people are continually manufacturing corona spike protein, from the viral genes which have been permanently incorporated into their genetic codes.
It could be said, in defense of the genetics-based-vaccine lobby, that since infection with whole, functional coronavirus clearly appears capable of transforming the human genetic code, causing our cells to forever manufacture the viral spike protein, there may therefore be some justification in mimicking this natural transformation via an unnatural RNA vaccine.
In condemnation of that lobby, however, we cannot overlook the obviously unwarranted assurances of vaccine manufacturers that alteration of our genetic code “will not happen.” Such a statement casts doubt on (a) their competence in their own field, and (b) their willingness to accept the consequences of their own actions.
Moreover, reverse transcription is a known means of normal human chromosome-to-chromosome gene mobility, a fascinating process whose study goes back to the pioneering workof Barbara McClintock in the 1930s. It has thus been well-known, for the better part of a century, that the effects of moving genes around will very much depend on where they are moved, and on exactly and precisely what is moved.
In the case of the current vaccine-borne corona spike protein gene, no one has any clue as to where in our genomes it will wind up, or what it will do when it gets there.
There is a corona vaccine, Novavax, which contains no genetic material at all (i.e., no DNA or RNA), but rather consists solely of the corona spike protein. Of all the available vaccines, this is the one least likely to cause human genetic harm. But almost no one gets it, because it’s not available in most countries. Why not?
There are also at least two corona vaccines (Sinopharm, Sinovac) which are made from whole inactivated virus, analogous to the polio vaccines of the 20th century. This is a tried and tested form of technology, but very few people get those vaccines either.
Instead, we’re all being pressured into taking hastily prepared genetic vaccines, which are likely to transform our heredity, permanently. Is there any reason for this, other than countless billions of dollars in windfall profits?
It is my view that the massive and barely studied global human genetic experiment going on right now is the biological equivalent of a drunk driver, speeding down the highway with impunity at 60 mph — at night without headlights — because he says that “he knows the road.”
Most sensible people are wary about “GMO,” even in food. Now we’re going to genetically modify ourselves? Why? What madness is this?
Ken Biegeleisen, M.D., Ph.D., has studied virology and is the author of multiple studies on virology and DNA/protein structure.