
Current Lyme Disease Research Shows These 6 New Developments
https://www.bustle.com/p/current-lyme-disease-research-shows-these-6-new-developments-17140501
Current Lyme Disease Research Shows These 6 New Developments

Vitalii Matokha/Shutterstock
Lyme disease is carried by ticks, and is a pretty well-known problem — around 300,000 cases are likely diagnosed in the US every year, according to the Center for Disease Control and Prevention — but there’s still a lot we don’t know about it. Lyme disease is more complex than it looks, and the first few months of 2019 have brought some studies that are changing our understanding of tick-borne diseases and Lyme.
People with Lyme disease contract it from the bite of a tick infected with a particular bacterium, often after traveling through tick-friendly areas like forests and prairies, and it can cause issues like joint pain, flu-like symptoms and a distinctive bulls-eye rash (though you can have Lyme even if you don’t see a rash). It’s treated with antibiotics. However, between 10 and 20% of people who are bitten suffer from symptoms long after the disease has been treated, and scientists aren’t entirely sure why.
“Some scientists believe the bacterium can persist in the body, but others dismiss the idea. This dispute, combined with patients whom doctors often can’t help, has created a fractious field unlike almost any other,” noted Science in a review of Lyme disease research funding in 2019.
New science is helping to solve this conundrum, and cast more light on Lyme in general. Here’s where Lyme research stands right now.
1. We Know More About Post-Lyme Disorder — And How We Might Cure It

One of the biggest mysteries of Lyme disease is what’s called post-treatment Lyme disease syndrome (PTLDS). Why does treatment work on some people and not others? What makes PTLDS patients particularly vulnerable, and how can you treat it?
2019 has brought a few answers. Research by Johns Hopkins Medicine has revealed that people with PTLDS have a particular kind of brain inflammation, and that it’s probably the source of their high inflammation levels in general — and the cause of a host of symptoms. This is a new discovery; before this study, nobody knew what was causing people with PTLDS to have elevated inflammation.
There’s hope for treatment of PTLDS too; a three-antibiotic ‘cocktail’, also formulated by scientists at Johns Hopkins, has shown some serious promise for treating slow-growing Lyme bacteria. These ‘persister’ bacteria, according to their theory, might be missed in the first treatment of Lyme disease and cause symptoms to last for months and years — but the cocktail, when it was given to infected mice, cleared up the problem totally. It needs to be given human trials, but it’s a promising lead.
2. Lyme Disease Is Expected To Increase Due To Climate Change
Lyme disease research is accelerating, and that’s good news — because experts in 2019 warned that as climates warm worldwide, it’ll become more common. The European Congress of Clinical Microbiology & Infectious Diseases noted that mosquito- and tick-borne illnesses worldwide, from Lyme to malaria, will probably infect more people worldwide. Dr Giovanni Rezza, Director of the Department of Infectious Diseases at the Istituto Superiore di Sanitá in Rome, said in a press release:
“The stark reality is that longer hot seasons will enlarge the seasonal window for the potential spread of vector-borne diseases and favor larger outbreaks.”
3. We Now Know The Grass Length In Your Garden Doesn’t Matter

Concerned that your backyard is a breeding-ground for dangerous ticks bearing Lyme bites — because you don’t mow it often enough? Research published in PLOS One in 2019 found that it might not actually matter. “We tested the hypothesis thatlawn mowing frequency influences tick occurrence,” the scientists explain in the study. They studied tick levels in 16 yards with varying mowing frequency in a region known for ticks, and found that there were no ticks at all. None. Zero.
“Promoting frequent mowing (i.e., shorter lawns) and the removal of grass clippings could have minimal impacts on tick microhabitats, but is consequential for beneficial wildlife and other ecosystem services associated with urban biodiversity,” they explain. Many species of endangered bee, for instance, like longer grass, so a bit of length is actually preferable.
4. Machine Learning Is Helping Us Diagnose Lyme Disease
Research published in Nature in 2019 reveals that machine learning — the principle behind artificial intelligence — can help understand Lyme disease, given that its symptoms in individuals can be radically different. The study tracked the medical records of Lyme disease patients at Mount Sinai hospital in New York, and found that using machine learning, it could predict comorbidities — illnesses that showed up at the same time – and what conditions and disorders might show up in certain people and not others as they recovered (or, in the case of PTLDS patients, didn’t). The aim, the study said, was to create a framework that could help individual treatment plans for Lyme disease patients, rather than going for a one-size-fits-all approach.
5. We Know More About How The Bacteria Itself Survives
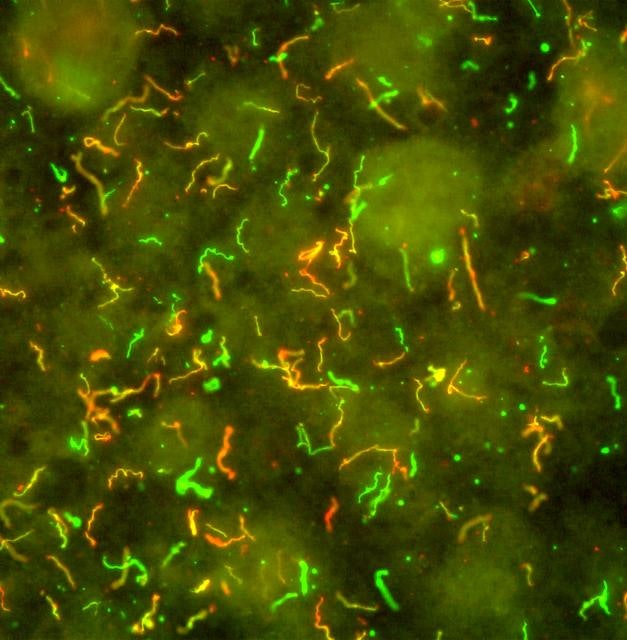
National Institute of Allergy and Infectious Diseases/Wikimedia Commons
The bacterium behind Lyme disease is called Borrelia burgdorferi, and it’s what’s transmitted into your system by an infected tick when it bites you. Research in 2019 by Connecticut scientists has found that Lyme disease bacteria have a very particular shape and structure that makes them dependent on peptides to function. They obtain these peptides from animal hosts like mammals, including, yes, humans. Without them, a Lyme disease bacterium doesn’t survive; with them, it thrives. Figuring out how to disable that mechanism might mean that one day, in the future, we can stop Lyme bacteria in their tracks.
6. ‘Persister’ Bacteria Might Be Killed By Plant-Based Treatments
In the future, we may be treating Lyme disease with treatments derived from garlic, cinnamon and cumin. That’s the interesting conclusion from a groundbreaking study from Johns Hopkins, one of the most important Lyme disease research centers worldwide. In late 2018 they published results showing that, in petri dishes in their labs, essential oils derived from 11 different natural sources — garlic, pimento, cumin, palm rose, cinnamon bark, myrrh, hedychium ginger flowers, torchwood, thyme, mountain pepper, and lemon eucalyptus — that were hugely effective against Lyme disease bacteria. More effective, in fact, than standard antibiotics.
“We found that these essential oils were even better at killing the ‘persister’ forms of Lyme bacteria than standard Lyme antibiotics,” lead study author Ying Zhang said in a press release. This doesn’t mean that Lyme disease patients should give up their antibiotics for inhaling or swallowing natural oils; for one thing, that’s likely dangerous, and for another, exposure in a petri dish is very different to life in the human body. It will take a long time before we know whether this can be replicated in medication form; right now, antibiotics are still the best way forward.
The mysteries surrounding Lyme disease and its persistent form are still complex, but there’s hope that new treatments will be developed — and that we’ll finally get ahead of this disease as it becomes more common worldwide.
____________________
**Comment**
The science isn’t settled on ALL the ways Lyme can be transmitted, despite what authorities say: https://madisonarealymesupportgroup.com/2019/04/02/transmission-of-lyme-disease-lida-mattman-phd/
While the rash means you HAVE Lyme, not having the rash means nothing. Anywhere from 27-80% get the rash depending upon who’s counting: https://madisonarealymesupportgroup.com/2019/02/21/lyme-disease-dont-wait-for-blood-tests-where-patients-have-bullseye-rash/ See comment after article.
This 10-20% with continuing symptoms is a falsely skewed number. A microbiologist explains in this article that it’s actually around 60%: https://madisonarealymesupportgroup.com/2019/02/25/medical-stalemate-what-causes-continuing-symptoms-after-lyme-treatment/
Key quote:
10-20% of Lyme disease patients who are promptly diagnosed and treated with an antibiotic within the first few weeks of infection, still end up with chronic disease. This is PTLDS.
30-40% of Lyme disease patients who have been infected for weeks to months before getting diagnosed, and THEN treated with an antibiotic, still end up with a chronic disease. This subgroup has no specific label but it has been referred to as “chronic Lyme disease,” or CLD.
Combining these two subgroups implies that up to 60% of people with Lyme disease will experience chronic illness as a result of this tick-borne disease.
Climate change has been disproven regarding tick and pathogen proliferation: https://madisonarealymesupportgroup.com/2018/08/13/study-shows-lyme-not-propelled-by-climate-change/
Studying the mowing patterns of 16 laws in ONE area of the country does not mean the science is settled. Mow your lawn. It just makes logical sense when you understand ticks love humidity. I seriously wish they’d take this type of research funding and apply it to testing, treatments, and transmission studies for practical information patients & doctors.
We don’t need the help of machines as much as we need doctors to pull their heads out of the sand.
Regarding ‘we know more about the bacterium’ – not until you deal with the pleomorphism (shape shifting) ability of Bb, as well as the fact many are polymicrobially (numerous pathogens) infected. These issues change the entire scope of this illness. For more background on this: https://madisonarealymesupportgroup.com/2019/04/29/is-the-sky-truly-going-to-fall-for-patients-with-the-untreatable-form-of-lyme-disease/
Many desperate patients out here in Lyme-land have tried a number of plant-based treatments on our own. While I’ve personally taken internal essential oils (plant based concentrates of herbs), they did NOT tackle this beast. I relapsed on them. They may work for a select subset of patients and they very well may be a great choice once a person has reached remission, but don’t bank on them for front-line treatment.
Just being real.

 Opinions expressed by contributors are their own.
Opinions expressed by contributors are their own.


{kind=link}
{kind=link}
.jpg){kind=link}