Avid Hiker Meets Bad Bug, Ends Up With Babesiosis
Avid hiker meets bad bug, ends up with babesiosis
Dear Dr. Roach • I am an avid hiker, and I live in an area with lots of Lyme disease. I recently developed some fever, headache, shaking chills and dark urine, and just felt awful. My doctor did some blood tests and said I had Babesia and/or Anaplasma. Are these related to Lyme disease? — I.J.M.
Answer • Like Lyme disease, babesiosis (caused usually by Babesia microti) and anaplasmosis (caused by Anaplasma phagocytophilium) can be spread by the bite of the deer tick, Ixodes scapularis, but neither bacteria species is related to Borrelia burgdorferi, the cause of Lyme disease. These diseases are not well-known by most people, nor even by many general doctors outside the areas where they are common, such as Wisconsin and Connecticut.
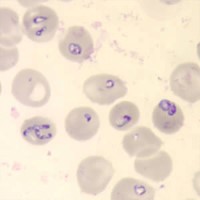
Babesiosis causes fever as high as 105.6 F, fatigue and feeling unwell. Dark urine is occasionally present. There are nonspecific lab findings, such as anemia and low platelet counts, but the diagnosis is confirmed by seeing the bacteria inside the red blood cells or by sophisticated blood testing (PCR). Treatment is with azithromycin and atovaquone.
Anaplasmosis has a generally lower fever, muscle aches, headache, chills and the same feeling of being unwell (called “malaise” in medical literature). Blood counts frequently show low white blood cell counts. The diagnosis is made by antibody or PCR testing, but treatment is usually started in the appropriate setting even before positive results. Treatment is with doxycycline.
Tickborne diseases may exist at the same time, so consideration must be given to people having both anaplasmosis and babesiosis, with or without Lyme disease.Doxycycline treatment for anaplasmosis also treats early Lyme disease, but does not treat babesiosis.
Both anaplasmosis and babesiosis can be very severe in people with immune system disease, such as HIV or an organ transplant. Older people are also at higher risk for severe disease.
Readers may email questions to ToYourGoodHealth@med.cornell.edu or send mail to 628 Virginia Dr., Orlando, FL 32803.
________________
**Comment**
This article reminds us of issues that demand answers:
- Why does mainstream medicine STILL know so little about tick-borne diseases after 40 years? https://madisonarealymesupportgroup.com/2019/08/22/early-diagnosis-necessitates-lyme-savvy-doctors/
- Why is testing STILL being used that is so unreliable after 40 years? https://madisonarealymesupportgroup.com/2019/08/05/controversies-challenges-in-treating-lyme-other-tick-borne-diseases/
- Please notice the doctor’s wise usage of “usually caused by?” This is wise because it could be one of a number of strains of Babesia.
- Please notice the the doctor’s wise explanation that a tick bite can transmit a whole host of pathogens – not just Lyme and sometimes not Lyme at all. This issue is what is completely being neglected in mainstream medicine because doctors aren’t looking at all for any of these coinfections that can come with or without Lyme. Since testing is abysmal for ALL of them, they should be educated in symptomology since diagnosis has always been and still is a clinical diagnosis. Testing is not accurate and should not be the sole means of diagnosis.
- Little research has been done on concurrent infection & what it does to the body and how it affects testing: https://madisonarealymesupportgroup.com/2018/10/30/study-shows-lyme-msids-patients-infected-with-many-pathogens-and-explains-why-we-are-so-sick/ But this recent study shows by Garg et al. shows a 85% probability for multiple infections including not only tick-borne pathogens but also opportunistic microbes such as EBV and other viruses. Mainstream medicine isn’t touching this with a ten foot pole.
- The good doctor points out that anaplasmosis and babesiosis can be very severe in people with compromised immune systems. I believe tick borne illness compromises the immune system greatly and it’s only logical to conclude that concurrent infection with numerous pathogens do so even more. Add a few opportunistic infections like Chlamydia and EBV, and you have a patient as sick as a dog: https://madisonarealymesupportgroup.com/2016/10/07/chlamydia-like-organisms-found-in-ticks/, https://madisonarealymesupportgroup.com/2017/04/11/diagnosed-with-ebv-had-lyme/ This is why patients are so sick and why standard mono therapy often doesn’t work.
Taking into account the totality of these issues presents an entirely different picture than what authorities such as the IDSA and CDC present.
This is often a complex illness with many moving parts which necessitates various drugs of longer duration than currently being used.
The CDC/IDSA “One size fits all” approach just doesn’t work. Until authorities take into account these variables and allow doctors to treat patients accordingly, it’s a losing battle – and make no mistake about it – it’s the patients who loose.