
CDC Playbook: Learning From Lyme

April 25, 2020
By Alicia Cashman MS, Lyme patient and advocate
While most of the world is staggering with newly imposed social distancing measures, worrying about viruses and how to bolster the immune system, chronic Lyme patients simply carry on doing these things daily. They’ve been isolated for some time – either to avoid illness due to being immunocompromised or because they were forced into exile by authorities who tell them the illness they are struggling with simply doesn’t exist. In time, family and friends become more and more distant because they tend to believe the authorities. Authorities, after all, are honest and are looking after public health – aren’t they?
They say history repeats itself, which appears to be the case regarding COVID-19 when you study the sordid history of how Lyme disease has been and continues to be handled.
The CDC Insists Upon Using Its Own Tests
Due to decisions made at a conference in Michigan, serology testing criteria for Lyme Disease were purposely manipulated for vaccine development. To this day the CDC insists upon its own two-tiered testing which research has proven is abysmal and misses a vast majority of cases. It can’t distinguish between active, past, or reinfection. It has now been removed, but the CDC website used to call specialized CLIA certified labs testing for tick-borne illness, “home-brewed.” I personally heard a pediatrician use those exact words at the Wisconsin State Capital in his effort of delegitimatizing patients who are forced to go to specially trained doctors using these labs to get diagnosed and proper treatment. This history is disturbing in and of itself but should particularly concern us in light of current events.
The CDC also insisted upon their own COVID-19 tests. It was just discovered that CDC COVID-19 tests were initially contaminated with COVID-19 – making ALL numbers based upon those tests absolutely worthless. COVID-19 laced tests were also found in the UK. Due to contamination, which they state on their website is a “problem with a reagent,” the entire United States is in lockdown. Had accurate testing been accepted by the CDC from the WHO from the start, authorities would have had accurate data to base decisions upon. This article states there are only 12 labs outside the CDC with the capability to test for the virus; however, as of the beginning of March, they hadn’t received FDA authorization to do their own testing. The CDC website states the following:
“This message is to remind clinical laboratories that this is currently the only EUA assay for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes COVID-19. Any laboratory that is not designated by CDC as a qualified laboratory and is implementing a COVID-19 diagnostic test other than the CDC EUA assay must contact the FDA to obtain an EUA before any COVID-19 diagnostic testing may be performed in their facilities.”
Compare that statement with the following:
“The conference proceedings recommended a two-test methodology using a sensitive enzyme immunoassay (EIA) or immunofluorescence assay as a first test, followed by a western immunoblot assay for specimens yielding positive or equivocal results (1,2).
On July 29, 2019, FDA cleared several Lyme disease serologic assays with new indications for use based on a modified two-test methodology (4). The modified methodology uses a second EIA in place of a western immunoblot assay. Clearance by FDA of the new Lyme disease assays indicates that test performance has been evaluated and is ‘substantially equivalent to or better than’ a legally marketed predicate test.“
In other words, you better use our tests. If you think that FDA cleared tests are effective, think again. The CDC has monopolized Lyme testing since the beginning of time, dooming patients to a life-time of suffering.
This article states that only two government agencies are required by law to be “patient-centered,” the FDA and the Patient Centered Outcomes Research Institute (PCORI), yet Lyme patients continue to experience false negative results on CDC 2-tiered testing. Negative results means no diagnosis and no treatment. Patients and advocates have complained profusely with no change in testing.
The reason for insisting upon their own tests become clear when you go down rabbit-holes to discover they own patents on nearly everything surrounding the diseases they have tests for. Please also see ConflictReport. Dr. Fauci, director of NIAID, and a leader in the Corona Task Force has numerous patents, and a long list of conflicts of interest.
- Journalist Mary Beth Pfeiffer summarizes CDC testing incompetence.
- James Lyons Weiler, Phd also reveals the CDC’s testing fiasco. He knows that of which he speaks as he attempted to have the CDC test his own test for Ebola. Let’s just say he was promptly rebuffed.
- Currently, a pathologist is suing the CDC for their willful suppression of direct detecting methods.
- Professor Lane hit the same brick wall regarding testing.
- Regarding COVID testing, the president of Tanzania (PhD Chemistry) punked the WHO by sending in goat, fruit, and motor-oil samples to be tested for COVID-19. Half came back positive!
- The creator of the PCR states it was never created to diagnose patients but for research and manufacturing purposes.
- Dr. David Rasnick, bio-chemist, protease developer, and former founder of an EM lab called Viral Forensics states,“I’m skeptical that a PRC test is ever true.” When asked his advice for people wanting to be tested for COVID-19, he said:
“DON’T DO IT…NO HEALTHY PERSON SHOULD BE TESTED. IT MEANS NOTHING BUT IT CAN DESTROY YOUR LIFE, MAKE YOU ABSOLUTELY MISERABLE.”
- According to David Crowe, Canadian researcher with degrees in biology and mathematics, host of The Infectious Myth podcast, and President of the think-tank Rethinking AIDS:
“The first thing to know is that the test is not binary,” he said. “In fact, I don’t think there are any tests for infectious disease that are positive or negative. What they do is they take some kind of a continuum and they arbitrarily say this point is the difference between positive and negative.”
Further, and more importantly, COVID testing does not detect SARS-COV-2 due to the fact the virus has not been isolated/purified from all else. You can’t test for something specific if you don’t have that information. COVID testing is not specific to a particular virus people have tested positive, then negative, then positive within hours or days. The test simply picks up viral fragments – some of which are completely dead and benign – not causing illness at all, and some are from other strains of coronaviruses such as the common cold, but it’s all being falsely labeled COVID-19 – further inflating case numbers and fear.
Lastly, there’s the very important issue of PCR cycle threshold, which was set at 40 (although this varied from lab to lab. Experts have weighed in stating a PCR cycle of 40 is far too sensitive and that it should be set much lower – around 30. Cases plummeted when the cycle threshold was lowered proving this fact. What is frightening about this is health ‘authorities’ can manipulate this cycle threshold for their own nefarious reasons.
This exact same fact is true with Lyme/MSIDS testing as well and is why research shows a majority do not test positive.
The CDC wants their own tests & patents so they can create their own vaccines and drugs they will profit from.
A vaccine called Lymerix caused Lyme-like symptoms in many. In fact, it can be directly linked to 222 deaths and hundreds of adverse reactions, and these are only the ones that were recorded.
The CDC to-date hasn’t even attempted to address the immune issues caused by Lymerix. They just deny it ever happened. In fact, another Lyme vaccine is in the works which still uses the same OspA component which is attributed with problems in the first human vaccine.
Fool me once, shame on you – fool me twice, shame on me.
COVID-19 vaccines have been fast-tracked thereby bypassing important safety studies. Dr. Hotez, a vaccine researcher, is on record stating previous respiratory vaccines caused “paradoxical immune enhancement“:
James Lyons Weiler, PhD also gives the following chilling prediction:
When Phase I trials become Phase II trials people will start getting infected w/SARS-CoV-2 following vaccination and start dying at even higher rates due to disease enhancement caused by Pathogenic Priming from SARS-CoV-2 vaccination – something the vaccine developers SHOULD have tested for in animal studies, but skipped.
Even the FDA is worried about potential risks of the PER C6 Ad5 technology (aborted fetal cells) within many COVID-19 vaccines, which not only has moral implications but oncogenicity and infectivity concerns. The vaccine also uses electricity to drive DNA into your cells.
A group of doctors recently wrote a paper about the emergency use authorized, fast-tracked COVID “vaccines” and state they are needless, ineffective and dangerous.
- needless because there are effective treatments (Scroll to comment section)
- ineffective because they don’t stop transmission or keep you from becoming ill
- dangerous due to causing: viral immune escape, an inevitable steep incline in future severe COVID cases, antibody-immune enhancement, a condition where the “vaccinated” suffer with more severe illness when exposed to the wild virus, but also any infection. There are also unsafe epitopes within the injections, and mounting reports of adverse reactions and deaths after these injections, which aren’t “vaccines.”
Faulty testing issues and the subsequent push for vaccines are uncannily similar between Lyme and COVID-19 and should strongly remind us that the CDC is a vaccine manufacturing company first and foremost – to the detriment of severely ill and desperate patients.
Why Should We Trust the CDC?
The question begging to be asked is why should anyone trust the CDC? Their track record speaks for itself. Even CDC scientists have formed a group exposing the corruption from within. They’ve also lied about flu figures for decades. The ACIP, a group within the CDC, votes “Yes” for new vaccines despite having no safety data. And let us never forget the CDC whistleblower who exposed that scientists were ordered to purposely destroy data showing that African-American males who got the MMR vaccine before 36 months had a 250% increase in autism diagnoses.
Recently, microbiologist Judy Mikovitz spoke out on the unethical behavior of Dr. Fauci, Director of the NIAID since 1984 and one of the lead members of the White House Coronavirus Task Force (NIAID and CDC are both under the HHS umbrella). Excerpt:
Dr Fauci ordered Mikovits to keep her mouth shut. When she refused, he illegally confiscated her work books and hard drives, drove her from government work + blackballed her from receiving NIH grants ending her science career.
For those of you who are unaware, Mikovits discovered that a mouse virus (XMRV) has contaminated vaccines all the way back to the 30’s. She believes the virus can be linked to diseases like chronic fatigue (CFS/ME), autism, Alzheimer’s, cancer, autoimmune, neuroimmune, central nervous system diseases, and even chronic Lyme disease. While retroviruses do not directly cause diseases by themselves they help to create acquired immune system deficiency (non-HIV AIDS) which in turn causes unrelenting inflammatory processes. Call it a trigger, in a perfect storm of events within the body allowing disease to occur.
You may ask why you’ve never heard of XMRV before. That’s because the CDC, NIH, FDA, and other government agencies covered it up. They didn’t want to worry you, and they certainly don’t want you to question their lucrative vaccines.
XMRV remains in American vaccines.
There is much evidence showing both COVID-19 and Lyme/MSIDS have been manipulated in a lab.
Ian Lipkin, aka The Virus Hunter, has been involved with both issues due to the urging of Dr. Fauci. He denies XMRV involvement in human disease, despite Mikovitz’s group being able to transmit it from patients’ T-cells to uninfected T-cells in the laboratory. He also denies COVID-19 is a lab-made, manipulated virus.
Despite his denial, the origin of COVID-19, after boomeranging around the globe, has returned to show strong evidence that it is most likely a manipulated virus for biowarfare purposes after all.
Excerpt:
After creating the synthetic virus, which they call SHC014, Zhengli and her coauthors write that they “next synthesized a full-length SHC014-CoV infectious clone based on the approach used for SARS-CoV.”24 Other papers Zhengli co-wrote focus on the transmission of coronaviruses from one species to another, according to the documentary.
Zhengli and her fellow researchers admit they used a “reverse genetics system” to generate “a chimeric virus expressing the spike of bat coronavirus,” raising legitimate fears that COVID-19 is also reverse-engineered, according to “Tracking Down the Origin of the Wuhan Virus.”
And the real clincher:
According to Mikovits, the S proteins seen on COVID-19 that make it so transmittable to humans come from “cutting and pasting of two different viruses” and the apparent insertion of four new genes could not have been generated from a natural “zoonotic transmission.”
They had to come from a medical, bioweapons or lab setting, says Mikovits. Other scientists in the film agree that COVID-19 is a re-engineered, laboratory-driven virus.
But we were warned about this months ago, and then again recently with even more damning details.
Lyme patients are also familiar with bioweaponization. Recently, Congressman Smith announced a DOD investigation on the bioweaponization of ticks. Tick researchers have gone on record admitting to experimenting on ticks and dropping them out of airplanes. And Kris Newby in her book “Bitten”, describes how a CIA operative dumped boxes full of crawling ticks over Cuba, returned home, and unwittingly infected his own newborn baby. Dr. William Burgdorfer, the discoverer of the causative agent of Lyme disease worked as a bioweapons researcher for the US military and worked in programs tasked with breeding ticks and infecting them with pathogens that cause human diseases.
Besides faulty testing, a thrust to create a vaccine at all costs, a tightly controlled narrative, and bioweaponization, there is also a similar smear campaign on successful clinical treatments in both Lyme disease and COVID-19.
The CDC Slanders Competing Treatments
Authorities have purposely thwarted IV therapy for Lyme patients in a recent MMWR paper. The short recap is that the CDC cherry-picked 5 cases that had poor outcomes using IV therapy and then wrote a paper scaring the bejesus out of doctors.
What’s interesting about the MMWR paper is that one of the authors, a CDC epidemiologist, allegedly solicited IDSA doctors for evidence of harm from IV antibiotic treatments, essentially bribing them by offering co-authorship of the report if anecdotes were used. No such solicitation was made for IV treatment success stories. The dangling carrot has been blatantly observed with COVID treatment. There has been hot debate on Lyme treatments for decades. The MMWR paper is only one example of bias which is embedded within the CDC. There are many success stories using IV therapy by a Wisconsin Doctor and IDSA founder who disagreed with his colleagues on how to treat Lyme disease.
Meanwhile, doctors are reporting in on the success of treatments for COVID-19, but the CDC, true to form, bad-mouths any treatment or tests, other than ones they orchestrate. Based upon the CDC’s casting a dark shadow upon treatments that even patients attribute to saving their lives, numerous states (MI, NV, NY) as well as France have banned their usage for COVID-19. It’s gotten so bad that judges are ordering hospitals to administer life-saving COVID treatment to dying patients because medical doctors kowtow to corrupt health ‘authorities’.
This tactic of politicizing clinically successful treatments is what the CDC/IDSA/NIH does. This article clearly shows the bantering common in mainstream media regarding COVID-19 treatment. The bi-partisan squabbling is tangible, and similar hit-pieces have been written about Lyme treatment for years. Lyme patients have had to straddle this polarized fence for over 40 years and this polarization continues unabated.
I was told by a front-line European doctor treating severely ill COVID-19 patients that hydroxychloroquine, commonly known as plaquenil, was used for over 70 years over the counter and was frequently given to travelers. Then, all of a sudden it became a prescription drug overnight, and now it’s being banned for use for COVID-19. This means doctors using it for COVID-19 will have their licenses revoked.
Scaring doctors and revoking their licenses is a common refrain for doctors treating Lyme disease. My own doctor had to pay over $50,000 in legal fees fighting this battle and it’s happening not only in the U.S. but around the world due to the Iron Curtain of the CDC.
There is no question that IV therapies as well as extended antibiotics for Lyme and hydroxychlorquine for COVID-19 have side effects. No one is denying this. What’s unconscionable is that ‘authorities’ zoom in on particular treatments and microscopically nit-pick due to ulterior motives. It becomes crystal clear that the motivation is to control the narrative, and protect special interests – not to safe-guard patients.
Everyone wants double blind, placebo, randomized controlled trials (RCT); however, in the case of Lyme disease, those studies are controlled by a cabal who continue to study only the acute phase of the disease with faulty parameters for entrance into their studies. Again, testing is rigged for a predetermined outcome and they exclude a large subset of patients who don’t meet their stringent criteria. Due to the complexity of Lyme/MSIDS, RTCs will never be done.
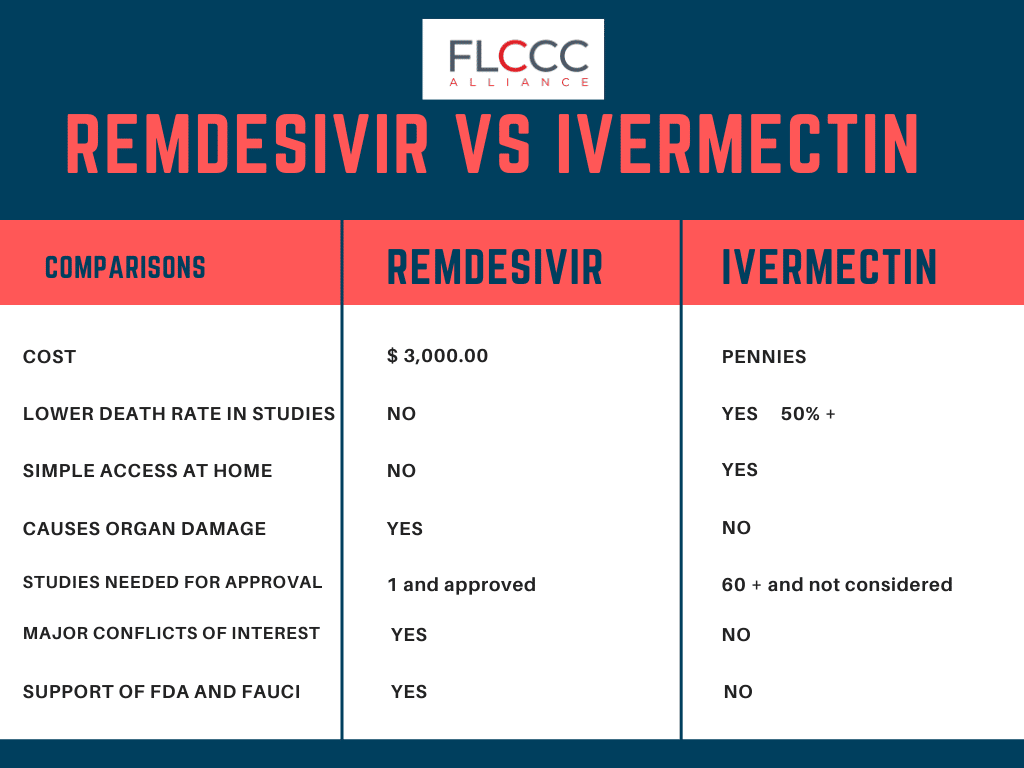
In the case of COVID-19, severe patients can quickly die, making those studies of little use in the present. Treatments are needed now, not in six months. Doctors and pharmacists go to school to learn about drugs and their interactions. How about authorities just let doctors do their jobs? I don’t see these authorities condemning cancer treatments which kill as many good cells as bad cells and cause horrific side-effects. Why the focus on HCQ, ivermectin, and benign treatments like vitamin D, C, zinc, and quercetin? This recent article explains why. In essence, the CDC is in bed with Gilead Science as nine of the experts on the NIH COVID-19 Panel recommending treatment options have disclosed financial support from Gilead. More dangling carrots.
Gilead Science created the anti-viral remdesivir which was unsuccessful for Ebola. They are now digging it out of the drug graveyard and pushing it for COVID-19 to make up for lost profits. They did this exact same thing with AZT, a chemotherapy drug which failed for leukemia, and repurposed it for HIV patients who didn’t even have symptoms! HCQ, even though it’s clinically showing great success, stands in the way of their chosen profitable, albeit dangerous treatment. Remdesivir is not without side-effects and only showed modest benefits against COVID-19 but this is the CDC’s “golden” treatment, therefore, everything said about it is positive while they bad-mouth HCQ a direct competitor.
It’s also important to understand that the NIH owns half of the Moderna COVID vaccine. Many other conflicts of interest exist regarding this unique injection technology.
Where the handling of the two diseases drastically departs; however, is in how seriously the CDC is handling COVID-19 by enacting what most declare to be draconian measures, while continuing to downplay Lyme disease. The learning curve for COVID-19 has been lightening fast in comparison to Lyme disease in that the conflicts of interest, the reliance upon faulty testing, and the polarization in the medical community on pretty much every aspect of the disease hasn’t budged in over 40 years.
What’s happening in the world today regarding COVID-19 is probably easier for Lyme patients to understand than the average person, but that doesn’t give them solace for the future. They will continue to wash their hands, do an entire laundry list of things to strengthen their immune systems, and will continue to be isolated. While the rest of the world returns to “normal” at some point, Lyme patients will continue living in a paradigm where the majority of doctors don’t even believe, test, or treat them, because the CDC has filled their heads with 40 year old unscientific, fraudulent dogma.



{kind=link}