Bartonella henselae is a relatively uncommon pathogen that can present as a serious disease in immunocompromised patients. We present a case of a 76-year-old man with stable chronic lymphocytic leukemia (CLL) who presented to the emergency department (ED) with an onset of right axillary lymphadenitis after recovering from a recent cat bite on the ipsilateral finger. Doppler ultrasound demonstrated an irregular, circumscribed 5cm x 4cm, hypoechoic mass with mild vascular flow consistent with an enlarged abnormal lymph node. The patient was diagnosed with cat scratch disease and discharged on oral antibiotics with spontaneous drainage of the purulent materials in subsequent outpatient oncology visits. This case highlights the classic presentation of this rare disease in an immunocompromised patient with feline contact. Early antibiotics should be considered for at-risk and immunocompromised patients due to low sensitivity and specificity for Bartonella serologic tests. CLL can also present with similar progressive lymphadenopathy with severe systemic symptoms and extranodal involvement that requires emergent oncologic interventions and diagnostic vigilance.
________________
**Comment**
Bartonella is NOT rare.
In this article, Dr. Mozayeni talks about Bartonella being one of the major co-infections of Lyme disease. It’s even more prevalent than Lyme, as there are many more ways to contract the disease (eg. flees, cats). In a study, that Dr. Breitschwerdt and Mozayeni published in The Journal of Emerging Diseases, about 60% of Lyme patients tested positive for Bartonella: https://madisonarealymesupportgroup.com/2016/01/03/bartonella-treatment/ If you want to know the likelihood of infection, please see the checklist within the article. Print it out and check how many symptoms you have. Take this with you to your doctor appointment and discuss the likelihood.
I’m glad this research article points out that testing is poor. This is true of each and every test for tick borne illness. This requires an educated and experienced practitioner to discover what patients are infected with. If you have tick borne illness, save your time and money and get to an ILADS trained doctor.
In my experience, I’ve found Bartonella to be harder to deal with than Lyme disease.
To describe a patient whose retinal findings suggestive of tick-borne disease but evaluations led to early diagnosis and treatment of human immunodeficiency virus (HIV) infection.
Observation
A young patient presented with bilateral uveitis, branch retinal artery occlusion and retinal findings suggestive of infective/inflammatory etiology. Laboratory evaluations revealed that the patient was positive for co-infection with Rickettsia conorii and Bartonella henselae. On further investigation, the patient tested positive for HIV infection. The patient was treated with doxycycline as well as highly active anti-retroviral therapy (HAART) to control both opportunistic infections as well as HIV infection.
Conclusion and Importance
Patients with HIV infection are at risk for multiple, simultaneous opportunistic co-infections, including those with tick-borne diseases.
Tickborne Triggered Seizure Disorder: Case Study of a Teenager with New Onset Seizure Disorder and the Neurological Impact of Tickborne Diseases
The Neurological impact of Bartonella and Rickettsia
This next case study is of an 18-year-old female who was adopted at the age of 5. Her adoptive mother described her as a malnourished premature baby who eventually received good foster care. This young lady was diagnosed with a growth hormone deficiency that was left untreated in her country of origin at the age of two. By the age of five, she was adopted and moved to the US with her American family. She was fully immunized twice, diagnosed with hypothyroidism and inadequate growth. By this time, an Endocrinologist was onboard and treating her thyroid and growth deficiencies. She seemed to rebound, reaching puberty by the age of 13. Life was stable for some time until January of 2016. She was nearly sixteen years old and developed sudden neuropsychiatric symptoms with acute confusion, severe obsessive-compulsive disorder, frequent urination, insomnia, auditory hallucinations, severe sensory issues, leg tremors and eventually catatonia. Given her acute changes, her mother rushed her to the Emergency Room for evaluation. EEG was negative and she was hospitalized for apparent acute psychosis treated with Risperdal and Ativan.
After her hospitalization she followed up with a well-known Neurologist who identified positive Mycoplasma and initiated a course of Azithromycin. By the fourth dose she began to return to her normal state and began sleeping again. She was treated for over a month with antibiotics and seemed stable.
There was a great deal of stress in the family, a close family member died and within two weeks she developed new onset grand mal seizures while sleeping. Another ER visit with a normal EEG at the time determined perhaps the stress and trauma of her family member’s death may have triggered the event.
In January 2018 she had another grand mal seizure early in the am. Her neurologist began medications to address. She had no additional seizure activity but noted increasing anxiety. By December 2018 she suffered another grand mal seizure.
Further evaluation by the neurologist showed negative Lyme screening only, viral panels negative, tick-borne co-infections were not obtained, thyroid studies, electrolytes and inflammatory markers were all within normal limits.
This patient presented to me in February 2019. Upon further evaluation she was found to have progressive muscle weakness, cognitive dysfunction ongoing psychiatric symptoms, tremors and noted random striae or “stretch-marks” that would appear and disappear all over her body. She stated that this had occurred since the age of fourteen. She admitted several evaluations with psychiatric acute hospital admission for escalating neuropsychological symptoms that included visual and auditory hallucinations, compulsions, rage, emotional lability, delusions, anxiety as well as the ongoing physical symptoms.Neuropsychological meds were ineffective. The patient upon presentation was taking high dose Depakote, gabapentin and folic acid to control her seizure activity.
Initial lab work up at my office showed an IGM positive Bartonella Henselae, Lyme Western Blot with an IGM indeterminate band 23-25 and IGG positive bands 18,23-25,28,31,34,39,41,45,and indeterminate bands 58 and 66. She also showed IGG positive Rickettsia and Anaplasma. She carried one copy of MTHFR A1298C and had significant GI bacteria overgrowth with Streptococcus, Citrobacter, Proteus and Bacillus.
She was started on a course of Azithromycin and Bactrim as well as biofilm busters and herbals. Two months later she reported significant improvements noting striae lightening, energy improvements, mood stability, resolution of hallucinations, and her sleep was improving. She noted ongoing body and hand tremors as well as struggles cognitively with word finding but was back in school full time.
We decided to continue the treatment course and repeat her bloodwork in two months as well as continue follow up with her Neurologist to monitor. By June the patient was feeling great. She began a Depakote wean with her Neurologist and graduated High School.
Her lab results showed improvements with Bartonella levels as well as GI bacterial overgrowth. Rickettsia antibodies lingered unchanged as did Lyme bands. I added to her regimen Doxycycline and Cefdinir as well as an antifungal and supportive herbals to prevent yeast.
This patient is still a work in progress, however what is important to note is her complete reversal of the neuropsychological symptoms once antibiotics were initiated as well as the ongoing, successful wean of seizure medications.
Bartonella and Rickettsia infections both have an affinity for the central nervous system. It is challenging to identify given their non-specific symptom presentation at times. Rickettsia isn’t well understood regarding brain parenchyma and central nervous system transmission. We know in mouse studies, Rickettsia and Bartonella both contribute to neuroinflammation which can contribute to acute psychological symptoms. We see this type of neurological process in classic PANS patients related to strep. Although I see the trend clinically, I don’t feel that autoimmune encephalopathy related to tick-borne infections in children and young adults is well documented.
My hope is thru case study presentations you’ll connect real world, everyday struggles of these vulnerable patients with the disease process. I strongly feel further exploration of autoimmune encephalopathy as it relates to Lyme and other Tickborne illnesses in pediatrics should be a collaborative effort with mental health practitioners and welcome those interested to contact me.
Patients with Bartonella species infection (bartonellosis) complain of a variety of nonspecific vision problems that can affect every function of the eye. Making diagnosis and treatment decisions even more difficult, these problems can be caused by a variety of other pathogens and diseases. Fortunately, many peer-reviewed case publications, especially in ophthalmology journals, are available that describe both common and uncommon eye symptoms caused by bartonellosis.
Documented links between Bartonella species infection and vision problems focus on Bartonella henselae (cat scratch disease) and Bartonella quintana (trench fever). B. henselae is associated with contact with animals and vectors, especially cats and fleas, while B. quintana is associated with body lice. Additional species implicated include B. elizabethae and B. grahamii.
Overview
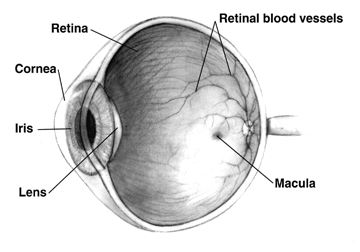
The eye consists of structures that focus light on nerve receptors at the back of the eye, nerves that feed into the optic nerve which connects to the brain, and a blood supply that connects through a central artery and vein into the body’s blood circulation. Bartonellosis can affect each of these parts of the eye.
Patients with bartonellosis-related eye problems may have symptoms in other organs as well that can help clarify whether the eye symptoms are caused by bartonellosis. Ophthalmologists and other physicians look for these additional signs because all of the eye conditions that can be caused by bartonellosis can be caused by a variety of bacteria and viruses, as well as other health conditions including autoimmune disorders.
It can be difficult to narrow down the possible causes of bartonellosis. Sometimes patients can’t remember any events that would have exposed them to Bartonella species. Other times the event, such as a cat scratch, may have occurred weeks to a month or more before symptoms appear and the patient may not think there is a connection. It can take detailed questioning by physicians to identify the possibility of Bartonella species exposure.
Structural Eye Symptoms
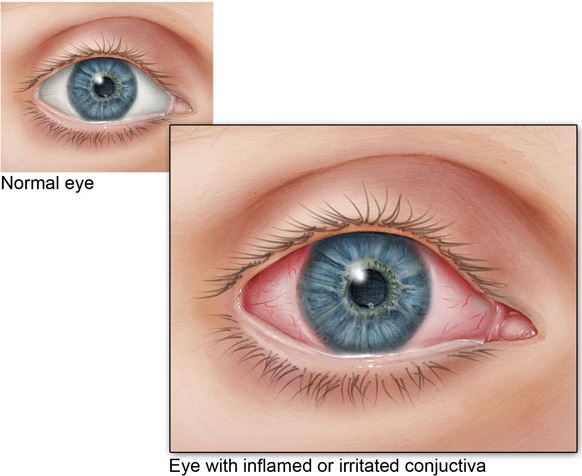
The most common way bartonellosis is seen in the eye is called Parinaud oculoglandular syndrome (POGS). About five percent of patients with acute cat scratch disease have this syndrome, which is characterized by follicular conjunctivitis (pink eye) with swollen lymph nodes nearby. It is often accompanied by a fever, and there may be bumps on the eyelid. Other symptoms known to be caused by bartonellosis, such as endocarditis (swelling of the inner lining of the heart), may also indicate that bartonellosis should be suspected.
Conjunctivitis results in easily seen inflammation of the usually white part of the eye (Source: CDC).
Inflammation of the middle layer of the structure that surrounds the eyeball is called uveitis. Uveitis causes redness of the eye and can cause light sensitivity, pain and floaters. Uveitis is sometimes associated with bartonellosis.
While case reports of eye symptoms caused by bartonellosis generally describe a sudden-onset condition, one case report describes a woman who had symptoms of bartonellosis in various body organs for more than five years, including chronic conjunctivitis (pink eye). She had multiple tests and treatments over that time including a Bartonella species test that was positive but considered nonspecific. It was only after other treatments didn’t work that antibiotics were administered. The antibiotics resolved her various symptoms.
Neurological Eye Symptoms
Neuroretinitis, an inflammation of the optic nerve head, occurs in about 2% of people with cat scratch disease (acute Bartonella henselae infection). Two-thirds of cases of neuroretinitis are caused by bartonellosis.
Neuroretinitis is usually characterized by sudden, complete vision loss and swelling that creates a star pattern in the macula (the light-sensitive tissue at the back of the eye that feeds information into the optic nerve). Though this is the typical case of neuroretinitis caused by bartonellosis, it can vary greatly. It can cause changes such as seeing odd shapes or colors Furthermore, case reports have included people who lose their vision with no other symptoms, have blurry vision with a headache, and more.
Treatment can usually, but not always, restore vision, but it can take months to resolve and there can still be long-term consequences. Complications can also occur. In one case, a child was diagnosed with neuroretinitis. Treatment was started six weeks after the diagnosis, but his vision in one eye got worse. After treatment, a full-thickness macular hole was discovered. The hole was monitored and resolved after six months.
Vascular Eye Symptoms
The eye has an important network of tiny blood vessels that provide nourishment to the tissue, but unnecessary growth of new capillaries can lead to a range of symptoms such as vision problems. Vasoproliferation (irregular growth of new blood vessels) may be more common in immunocompromised people, such as those being treated with chemotherapy products. These symptoms can be observed on the skin and in the liver and spleen and may also occur in the eye.
Tiny blood vessels in the eyes supply nutrients to cells. In the above image, larger retinal blood vessels can be seen (Source: NIH).
Vasoproliferative symptoms seem to be caused by vascular endothelial growth factor (VEGF) stimulated by bartonellosis. More research on the relationship between VEGF and bartonellosis is needed. Meanwhile, anti-VEGF agents have been used to treat vasoproliferative eye symptoms.
Conclusion
Bartonellosis can affect every part of the eye, and symptoms can be sudden and severe. Diagnosis and treatment decisions are complicated by other pathogens and diseases that can cause similar symptoms. It is important for patients and physicians to be aware of any prior animal or insect exposure that may indicate Bartonella infection. Considering additional systemic symptoms of bartonellosis may also help to clarify the diagnosis.
Learn more about bartonellosis and the testing that Galaxy Diagnostics offers here.
References
Kalogeropoulos, C. et al. (2011). Bartonella and intraocular inflammation: A series of cases and review of literature. Clinical Ophthalmology, 5, 817-829. doi:10.2147/OPTH.S20157 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3130920/
Woo, M. et al. (2018). A case of retinal vessel occlusion caused by Bartonella infection. Journal of Korean Medical Science, 33(47), e297. doi:10.3346/jkms.2018.33.e297 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6236082/
Fairbanks, A. M. et al. (2019). Treatment strategies for neuroretinitis: Current options and emerging therapies. Current Treatment Options in Neurology, 21(8), 36. doi:10.1007/s11940-019-0579-0 https://www.ncbi.nlm.nih.gov/pubmed/31278547
Michel, Z. et al. (2019). Multimodal imaging of two unconventional cases of Bartonella neuroretinitis [epub ahead of print]. Retinal Cases & Brief Reports. doi:10.1097/ICB.0000000000000893 https://www.ncbi.nlm.nih.gov/pubmed/31348120
Gunzenhauser, R. C. et al. (2019). The development and spontaneous resolution of a full-thickness macular hole in Bartonella henselae neuroretinitis in a 12-year-old boy. American Journal of Ophthalmology Case Reports, 15, 100515. doi:10.1016/j.ajoc.2019.100515 https://www.ncbi.nlm.nih.gov/pubmed/31341998
Toumanidou, V. et al. (2017). Neuroretinitis secondary to Bartonella henselae in a patient with myelinated retinal nerve fibers: Diagnostic dilemmas and treatment. Ocular Immunology and Inflammation, 27(3), 396-398. doi:10.1080/09273948.2017.1409357 https://www.ncbi.nlm.nih.gov/pubmed/29283743
Mabra, D. et al. (2018). Ocular manifestations of bartonellosis. Current Opinion in Ophthalmology, 29(6), 582-587. doi:10.1097/ICU.0000000000000522 https://www.ncbi.nlm.nih.gov/pubmed/30124532
Beckerman, Z. et al. (2019). Rare presentation of endocarditis and mycotic brain aneurysm [epub ahead of print]. The Annals of Thoracic Surgery. doi:10.1016/j.athoracsur.2019.06.073 https://www.ncbi.nlm.nih.gov/pubmed/31425670
_________________
**Comment**
Another great article by Galaxy Lab. Please read the following article for more information on Bartonella, as various strains are suspected to be transmitted by ticks, mites, various flies and spiders, and other modes, and it is far more prevalent than thought: https://madisonarealymesupportgroup.com/2016/01/03/bartonella-treatment/ Fifteen species of gram-negative aerobic Bartonella are known to infect humans; however Dr. Ricardo Maggi’s statement is quite telling, “This case reinforces the hypothesis that any Bartonella species can cause human infection.”
Division of Pediatric and Congenital Cardiothoracic Surgery, Department of Surgery and Perioperative Care. Electronic address: zbeckerman@austin.utexas.edu.
2
Tecnologico de Monterrey, Escuela de Medicina y Ciencias de la Salud, Monterrey, Mexico; Division of Pediatric and Congenital Cardiothoracic Surgery, Department of Surgery and Perioperative Care.
3
Department of Pediatrics, University of Texas Dell Medical School, Dell Children’s Medical Center, Austin, Texas.
4
Division of Pediatric and Congenital Cardiothoracic Surgery, Department of Surgery and Perioperative Care; Department of Pediatrics, University of Texas Dell Medical School, Dell Children’s Medical Center, Austin, Texas.
Abstract
Bartonella endocarditis can be a very elusive diagnosis. The clinical manifestations can vary and, at times, include multiorgan involvement. This case report describes two patients presenting with multiorgan failure, cerebral mycotic aneurysms and valvular endocarditis secondary to Bartonella infection. The complex diagnosis, decision making, and surgical management are described.
________________
**Comment**
It’s unfortunate that once again the study authors choose the word “rare” regarding Bartonella and/or any tick-borne infection manifestations, as even the most hardened critics admit these pathogens are prevalent and can have highly variable presentations. It would have been much more appropriate that the authors would state it’s the first time these particular findings have been published rather than give people the impression something occurs rarely.
Again, please keep in mind that current 2-tiered CDC testing is based on blood tests that misses half of all cases and do not look for the organism but the body’s immune response (antibodies): https://madisonarealymesupportgroup.com/2018/12/16/laboratory-testing-for-lyme-disease/ Current CDC guidelines were created for surveillance purposes only but are being used diagnostically. All patients should be informed that they can still be infected despite a negative test.
There are going to be patients with heart symptoms that have an underlying tick-borne illness but test negatively (seronegative). These people are falling through the cracks of the medical symptom yet could be greatly helped with appropriate antimicrobial treatment. If you suspect you are one of these people or suspect others, please give the validated Horowitz questionnaire to them to take to their practitioner: https://madisonarealymesupportgroup.com/2017/09/05/empirical-validation-of-the-horowitz-questionnaire-for-suspected-lyme-disease/ It also takes an open mind and trained eye to diagnose these patients, and it can be Lyme, Baronella, or any one of many pathogens transmitted by ticks: https://madisonarealymesupportgroup.com/2019/08/22/early-diagnosis-necessitates-lyme-savvy-doctors/ I hope doctors are waking up to the growing need for education regarding the growing link between tick-borne illness and heart issues.

 3
3