LymeMIND: Looking Towards the Future
http://” data-wplink-url-error=”true”>a; gyroscope; picture-in-picture” allowfullscreen></iframe> Approx. 12 Min

https://www.lymedisease.org/mervine-coments-tbdwg-nov17/

Phyllis Mervine delivered the following remarks by telephone at the November 17 meeting of the Tick-Borne Disease Working Group.
Good morning. I am Phyllis Mervine, Founder and President of LymeDisease.org, the oldest Lyme patient advocacy nonprofit in the country.
I and other patients have submitted written and oral comments to the Working Group over the past few years. We have also served on subcommittees. I want to emphasize 5 points from these comments.
1. Pat Smith is one of my heroes, but no single person should have to carry the burden of representing the entire patient community on the Working Group. Please make sure more patients are represented next year. Patients deserve to have fair representation and strong voices on this group.
2. We also need more transparency in how Working Group members are picked. HHS ignored our petition of over 38 thousand signatures to remove Gene Shapiro. Dr. Shapiro has conflicts of interest and a long history of disrespectful conduct toward the Lyme community. He has served as an expert witness against ILADS doctors in medical board prosecutions and is a named defendant in a federal lawsuit that charges IDSA guidelines authors and insurance companies with conspiring to deny medical care to Lyme disease patients. Dr. Shapiro’s anti-patient bias on this Working Group has borne out our concerns about his participation. Patients deserve better.
3. Geographic limitations which hinder timely diagnosis should be removed. They make it more difficult for people in states the CDC labels “low endemic” to get diagnosed and treated. Northern California is a case in point. We’ve asked the CDC to revert to the county-based maps so high-risk counties within low-risk states can be identified more easily. We’ve asked the CDC to remove the geographic restrictions from their surveillance case definition to help patients to be diagnosed quickly and avoid chronic disease.
4. The CDC should not be taking sides between the IDSA and ILADS as they have been doing for years, in violation of federal guidelines about peer review. Most patients with chronic Lyme are treated by ILADS doctors because IDSA doesn’t provide any effective treatments for chronic Lyme. Let doctors know there are two standards of care.
And finally,
5. Tick-borne disease educational materials developed for doctors need to present the spectrum of scientific and clinical perspectives on tick-borne diseases, not just IDSA. The CDC should not take partisan positions in professional turf wars that benefit the IDSA to the detriment of sick patients.
Thank you for your attention.
By the way, my friend and neighbor with ALS, who I told you about in January, and who was belatedly diagnosed with tick-borne diseases, died in July. He was 72.
Phyllis Mervine has advocated for the rights of Lyme patients for more than 30 years.
___________________
For more letters to the TBDWG: https://madisonarealymesupportgroup.com/2020/11/06/the-proof-is-in-the-pudding-my-letter-to-the-tbdwg/
https://madisonarealymesupportgroup.com/2020/08/27/the-lyme-voices-you-didnt-hear-at-tbdwg-meeting/
https://www.bmj.com/content/371/bmj.m4425
BMJ 2020; 371 doi: https://doi.org/10.1136/bmj.m4425 (Published 13 November 2020)Cite this as: BMJ 2020;371:m4425
Politicians and governments are suppressing science. They do so in the public interest, they say, to accelerate availability of diagnostics and treatments. They do so to support innovation, to bring products to market at unprecedented speed. Both of these reasons are partly plausible; the greatest deceptions are founded in a grain of truth. But the underlying behaviour is troubling.
Science is being suppressed for political and financial gain. Covid-19 has unleashed state corruption on a grand scale, and it is harmful to public health.1 Politicians and industry are responsible for this opportunistic embezzlement. So too are scientists and health experts. The pandemic has revealed how the medical-political complex can be manipulated in an emergency—a time when it is even more important to safeguard science.
The UK’s pandemic response provides at least four examples of suppression of science or scientists. First, the membership, research, and deliberations of the Scientific Advisory Group for Emergencies (SAGE) were initially secret until a press leak forced transparency.2 The leak revealed inappropriate involvement of government advisers in SAGE, while exposing under-representation from public health, clinical care, women, and ethnic minorities. Indeed, the government was also recently ordered to release a 2016 report on deficiencies in pandemic preparedness, Operation Cygnus, following a verdict from the Information Commissioner’s Office.34
Next, a Public Health England report on covid-19 and inequalities. The report’s publication was delayed by England’s Department of Health; a section on ethnic minorities was initially withheld and then, following a public outcry, was published as part of a follow-up report.56 Authors from Public Health England were instructed not to talk to the media. Third, on 15 October, the editor of the Lancet complained that an author of a research paper, a UK government scientist, was blocked by the government from speaking to media because of a “difficult political landscape.”7
Now, a new example concerns the controversy over point-of-care antibody testing for covid-19.8 The prime minister’s Operation Moonshot depends on immediate and wide availability of accurate rapid diagnostic tests.9 It also depends on the questionable logic of mass screening—currently being trialled in Liverpool with a suboptimal PCR test.1011
The incident relates to research published this week by The BMJ, which finds that the government procured an antibody test that in real world tests falls well short of performance claims made by its manufacturers.1213 Researchers from Public Health England and collaborating institutions sensibly pushed to publish their study findings before the government committed to buying a million of these tests but were blocked by the health department and the prime minister’s office.14
Prior publication of research on a preprint server or a government website is compatible with The BMJ’s publication policy. As if to prove a point, Public Health England then unsuccessfully attempted to block The BMJ’s press release about the research paper.
Politicians often claim to follow the science, but that is a misleading oversimplification. Science is rarely absolute. It rarely applies to every setting or every population. It doesn’t make sense to slavishly follow science or evidence. A better approach is for politicians, the publicly appointed decision makers, to be informed and guided by science when they decide policy for their public. But even that approach retains public and professional trust only if science is available for scrutiny and free of political interference, and if the system is transparent and not compromised by conflicts of interest.
Suppression of science and scientists is not new or a peculiarly British phenomenon. In the US, President Trump’s government manipulated the Food and Drug Administration to hastily approve unproved drugs such as hydroxychloroquine and remdesivir.15 Globally, people, policies, and procurement are being corrupted by political and commercial agendas.16
The UK’s pandemic response relies too heavily on scientists and other government appointees with worrying competing interests, including shareholdings in companies that manufacture covid-19 diagnostic tests, treatments, and vaccines.17 Government appointees are able to ignore or cherry pick science—another form of misuse—and indulge in anti-competitive practices that favour their own products and those of friends and associates.18
How might science be safeguarded in these exceptional times? The first step is full disclosure of competing interests from government, politicians, scientific advisers, and appointees, such as the heads of test and trace, diagnostic test procurement, and vaccine delivery. The next step is full transparency about decision making systems, processes, and knowing who is accountable for what.
Once transparency and accountability are established as norms, individuals employed by government should ideally only work in areas unrelated to their competing interests. Expertise is possible without competing interests. If such a strict rule becomes impractical, minimum good practice is that people with competing interests must not be involved in decisions on products and policies in which they have a financial interest.
Such ill judged moves leave science, the media, and stock markets vulnerable to manipulation. Clear, open, and advance publication of the scientific basis for policy, procurements, and wonder drugs is a fundamental requirement.19
The stakes are high for politicians, scientific advisers, and government appointees. Their careers and bank balances may hinge on the decisions that they make. But they have a higher responsibility and duty to the public. Science is a public good. It doesn’t need to be followed blindly, but it does need to be fairly considered. Importantly, suppressing science, whether by delaying publication, cherry picking favourable research, or gagging scientists, is a danger to public health, causing deaths by exposing people to unsafe or ineffective interventions and preventing them from benefiting from better ones. When entangled with commercial decisions it is also maladministration of taxpayers’ money.
Politicisation of science was enthusiastically deployed by some of history’s worst autocrats and dictators, and it is now regrettably commonplace in democracies.20 The medical-political complex tends towards suppression of science to aggrandise and enrich those in power. And, as the powerful become more successful, richer, and further intoxicated with power, the inconvenient truths of science are suppressed. When good science is suppressed, people die.
Footnotes
Competing interests: I have read and understood BMJ policy on declaration of interests and have no relevant interests to declare.
Provenance and peer review: Commissioned; not externally peer reviewed.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
References
Bowing down to external forces to suppress and downplay results that don’t fit the accepted narrative is the ‘new norm’ in science. Prepare for more of it. This has been done for over 40 years with Lyme/MSIDS. Public ‘authorities’ just ignore research they don’t like & pretend it doesn’t exist.
https://www.lymedisease.org/torrey-idsa-insurance-settlement/
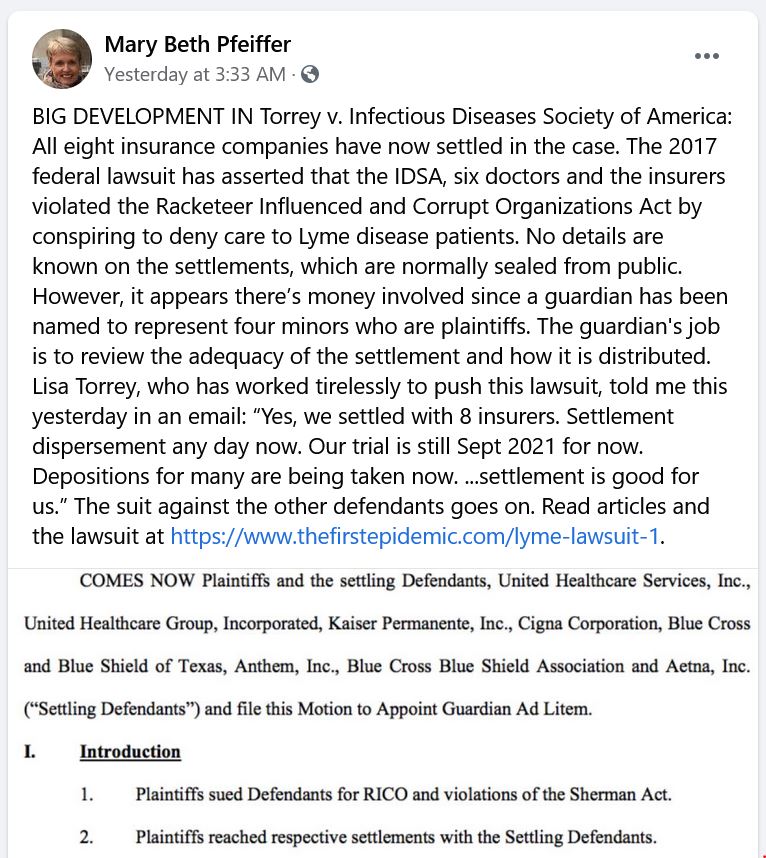
All eight insurance companies named in Torrey v. Infectious Diseases Society of America have settled the case, according to journalist Mary Beth Pfeiffer on Twitter.
That’s the federal lawsuit filed by a group of Lyme patients against the IDSA, six authors of the IDSA Lyme treatment guidelines, and the insurance companies.
The companies involved are:
The named individuals in the case are
As is typical in such circumstances, no details have been released. According to lead defendant Lisa Torrey, a trial date has been set for September 2021.
Please note that the 7 men listed make up The Cabal which continues to do faulty, biased research only on the acute stage of Lyme disease. Their studies are rigged to only accept those with EM rashes and positive blood serology testing which misses 70-86% of those infected. The studies have a short followup. They refuse to study the sickest patients who continue to be plagued with symptoms. They refuse to admit these people are even infected. To them these suffering patients are just imagining it.
https://www.medpagetoday.com/publichealthpolicy/generalprofessionalissues/89261? Go here for video
Following is a transcript of this video; note that errors are possible:
Rohin Francis, MBBS: Welcome back to yet another night shift. It’s Shift #4 and in a fit of narcissistic delirium I decided to search for one of my own publications, but I can’t actually see it without paying. The per-article price is about standard, £30 or $40.
If you’re writing a paper, you might reference 50 studies, which would be a huge expense. Luckily I get access through my university, who are in turn funded by me and other students through our fees and by the government. An establishment like UCL will pay something £10 to £12 million pounds a year for subscriptions to scientific journals, most of which belong to just five publishing companies. (See link for article)
Rohin Francis, MBBS, is an interventional cardiologist, internal medicine doctor, and university researcher who makes science videos and bad jokes. Offbeat topics you won’t find elsewhere, enriched with a government-mandated dose of humor. Trained in Cambridge; now PhD-ing in London.
__________________
**Comment**
Science journals have gotten away with one of the biggest monopolizing schemes in the world.
